F. F. Poordad
Authors and Disclosures
Posted: 08/18/2010; Alimentary Pharmacology & Therapeutics. 2010;31(12):1251-1257. © 2010 Blackwell Publishing
.
Discussion Only
Rapid virological response is an important and accurate positive predictor of SVR. For this reason, treatment duration can be shortened among patients who attain RVR without discernible declines in SVR rates.
.
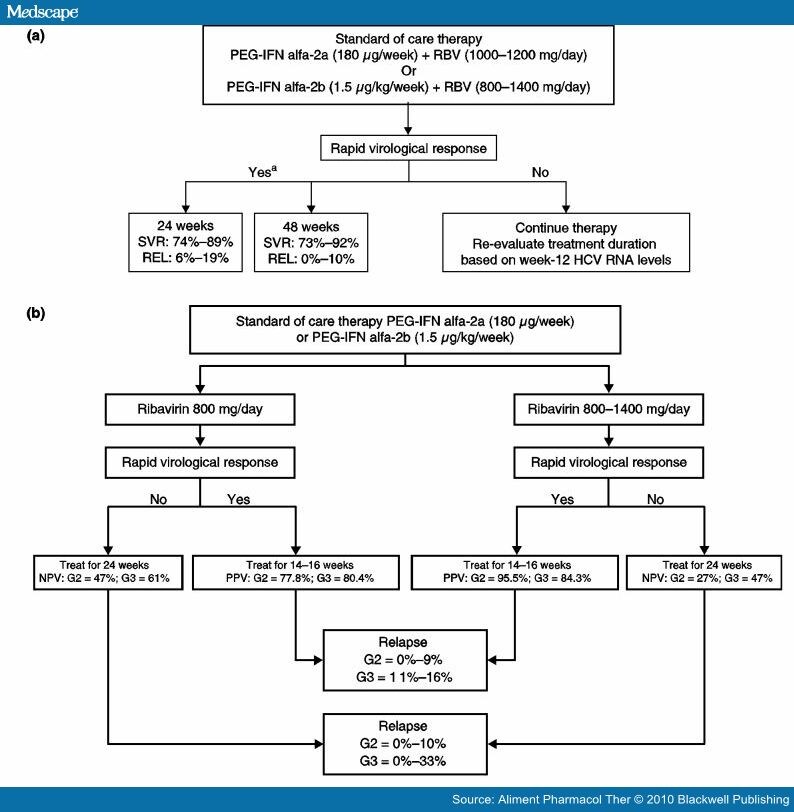
Results of this literature analysis suggest that treatment may be shortened from 48 to 24 weeks among G1 patients who attain RVR. This observation is consistent with the recommended use of PEG-IFN alfa in Europe, where there is an optional 24-week treatment duration for G1 patients with baseline viral load less then 600 000 IU/mL (PEG-IFN alfa-2b) or less then 800 000 IU/mL (PEG-IFN alfa-2a) who have undetectable HCV RNA at week 4 and who remain virus-free at week 24 (Figure 4).[34, 35] RVR is a less reliable predictor of treatment failure. Approximately 60% of G1 patients who do not attain RVR will not attain SVR when treated for 48 weeks. Thus, lack of RVR represents a setback in treatment progress, but does not represent grounds for withdrawing patients from therapy because approximately 40% of G1 patients who do not attain RVR will go on to attain SVR.
,.
Furthermore, in the present analysis, the sensitivity of assays used to define RVR varied widely across the included studies, with LLDs ranging from 50 to 600 IU/mL. However, we strongly advise that wherever possible, an assay with a LLD less then 50 IU/mL be used to define RVR, thus avoiding the erroneous classification of very low levels of HCV RNA as undetectable.
v
.

Enlarge Image)
j.
Figure 4.Predictive value of RVR in the treatment of (a) genotype 1 or (b) genotype 2/3 patients. PEG-IFN, pegylated interferon; REL, relapse; RBV, ribavirin; SVR, sustained virological response; WBD, weight-based dose. a
.
The decision to stop therapy at week 24 or to continue to week 48 might have been influenced by other disease characteristics, including baseline viral load, tolerability, adherence and patient preference.
.
Among G2 and G3 patients, the predictive value of RVR for SVR is dependent on treatment duration and ribavirin dosing. Treatment can be shortened from 24 weeks to 12–16 weeks in patients with RVR, but these data suggest it is preferable to use a weight-based ribavirin regimen alongside the reduced treatment duration. With a shortened treatment duration and a fixed 800-mg/day ribavirin dose, RVR is a weak predictor of SVR, but lack of RVR is a strong predictor of treatment failure. In contrast, RVR is a strong predictor of SVR, but lack of RVR is a weak predictor of treatment failure when a weight-based ribavirin dosing regimen is used for 24 weeks.
.What ribavirin dosing schedule should be used in G2 and G3 patients? At the outset of therapy, physicians must consider whether to initiate a standard fixed-dose[9] or a weight-based dosing regimen of ribavirin. Results of the present analysis indicate that RVR rates are comparable among G2/3 patients receiving weight-based ribavirin (68.8%) and fixed-dose ribavirin (65.5%). However, beyond week 4, our data suggest that the type of dosing chosen affects SVR rates (Figure 4).
.This pooled analysis suggests that for G2/3 patients who do not attain RVR, fixed-dose ribavirin can be continued for 24 weeks. However, these observations suggest that consideration may be given to adjusting ribavirin dose in G2/3 patients who are started on a fixed 800-mg/day dose and subsequently attain RVR and are thus selected for shortened treatment duration. For these patients, the clinician may elect to make no change to the fixed 800-mg/day dose, a strategy which, our data suggest, is associated with slightly lower PPV than if using weight-based ribavirin; or change to a weight-based ribavirin dosing, a strategy which would necessitate an increase in ribavirin dosing for some patients, but which is also associated with a high likelihood of SVR.
.
In the event of ribavirin-related toxicity arising from the increase in dose, ribavirin could be safely reduced back to 800 mg/day and treatment duration returned to the original 24 weeks. Alternatively, G2/3 patients could start with a weight-based ribavirin regimen.
.
This regimen would then be maintained for 12–16 weeks in patients who attain RVR. In patients who experience ribavirin-related toxicity, the dose could be reduced to 800 mg/day and treatment duration extended to the standard 24-week period. These approaches require prospective evaluation before any decisions can be made regarding the more effective regimen. PEG-IFN alfa-2a and PEG-IFN alfa-2b have different approved regimens for the treatment of G2/3 patients. In the United States and Europe, PEG-IFN alfa-2b is approved for the treatment of G2/3 patients when combined with a weight-based ribavirin schedule (800–1400 mg/day) for a period of 24 weeks.[34, 36]
.
In contrast, in the United States and Europe, PEG-IFN alfa-2a is approved when combined with ribavirin at a fixed dose of 800 mg/day, also for 24 weeks.[35, 37] However, European recommendations also indicate that a treatment period of 16 weeks (without any adjustment of ribavirin dose) may be considered with PEG-IFN alfa-2a in G2/3 patients with baseline viral load less then 800 000 IU/mL who have undetectable HCV RNA at week 4 that remains undetectable at week 16.[35]
.Several other questions remain to be prospectively evaluated. For example, prospective data are required to determine whether treatment duration can be shortened to 12 weeks[23] or whether more conservative 14-week[22] or 16-week[26] treatment durations offer improved outcomes. Furthermore, the relative merits of various weight-based ribavirin regimens also require assessment. Prospective comparison of the 'full' weight-based approach (800–1400 mg/day[22]) with less structured 800- to 1200-mg/day[26] or 1000- to 1200-mg/day[23] treatment is also of interest. Baseline viral load is also recognized as an important factor in determining appropriate treatment duration and studies have shown a close relationship between low baseline viral load and increasing likelihood of RVR, both in patients with G1 and with G2/3 infection.[16, 34]
.
However, a proportion of patients with high baseline viral load also attain RVR, with data indicating that 9.2% of G1 patients with baseline viral load more then 600 000 IU/mL will attain RVR.[16] Clearly, there is a strong association between baseline viral load and RVR, and further study is required to establish the degree of accuracy with which baseline viral load can predict RVR.
.
{kind=link}
The present analysis confirms the strong predictive value of RVR for SVR across the entire continuum of chronic hepatitis C disease and shows how the predictive value of RVR can fluctuate according to genotype, treatment duration and ribavirin regimen. However, SVR is not the only possible clinical outcome in patients who attain an EOT response.
.
Relapse is also emerging as an important clinical end point. Patients who have relapses after full-course therapy experience emotional strain related to the late failure of therapy. Recent data from the Hepatitis C Antiviral Long-term Treatment Against Cirrhosis (HALT-C) study showed significant declines in measures of physical and sexual functioning and general health (as assessed using the 36-item Short-Form Health Survey) in patients who experienced relapse compared with patients who attained SVR after re-treatment.[38]
.
Furthermore, maximum health care expenditure (to deliver a full course of therapy and manage side effects for the entire treatment period) is lost when patients experience relapse..
Although not confirmed through statistical analysis, the results of the present analysis strongly indicate a close relationship between RVR and relapse. Across all genotypes, relapse rates are generally higher among patients who do not attain RVR than among those who do, an observation that is consistent with the theory of continuously undetectable HCV RNA. Further studies are urgently required to understand the full pathobiology of relapse. Clinical focus on EOT response rate as a marker of efficacy is misleading and can create false hope of SVR among patients who attain undetectable HCV RNA late in their treatment course.
.
Of greater clinical value are early changes in HCV RNA, which can be used to tailor therapy according to each patient's response. Measures to mitigate relapse should begin early in therapy, when proactive control of influencing factors, such as ribavirin dosing and treatment duration, is possible. The belief that relapse occurs simply as a function of end-of-treatment viraemia represents a passive attitude to managing relapse and does not adequately take into account the on-treatment factors that can influence this treatment outcome..
Finally, while this analysis has focused on data regarding the role of RVR in the treatment of hepatitis C genotypes 1, 2 and 3 infections, there is also a limited amount of information available regarding the role of RVR in treating hepatitis C genotype 4. Ferenci et al. reported that 30 of 66 patients (45.5%) receiving PEG-IFN alfa-2a plus ribavirin attained RVR with a PPV of 86.7% when treated for 24 weeks.[19] Similarly, Kamal et al. found that 69 of 358 (19.3%) patients with G4 infection attained RVR when treated with PEG-IFN alfa-2b plus ribavirin and, as in the study by Ferenci et al., 86% of these patients attained SVR after a 24-week treatment duration.[39]
l
This study also included a control population in which 50 patients with G4 infection were treated for a fixed 48-week period. Among these 50 patients, eight attained RVR (16%) of whom seven attained SVR (88%) after 48 weeks of therapy, suggesting that there is no incremental benefit in extending treatment duration from 24 to 48 weeks in G4 patients with RVR.[39].
In conclusion, the present analysis confirms the importance of RVR in the individualized approach to the treatment of patients with chronic hepatitis C. RVR is a strong predictor of SVR and, as such, can be used to tailor treatment duration.
..
However, the results of this analysis confirm that RVR is a dynamic variable influenced by other factors. Therefore, the predictive value of RVR has to be appreciated in the context of treatment duration and treatment regimen. These findings confirm that a strong continuum exists throughout a course of treatment for chronic hepatitis C and the influence that an early event such as RVR can have on SVR and relapse rates. Controlled prospective studies are now warranted to evaluate these observations in a clinical setting
..
Complete Article
Abstract and Introduction
Free registration required
No comments:
Post a Comment