From Alimentary Pharmacology & Therapeutics
The Effects of Gut Flora Modulation using Prebiotics, Probiotics and Synbiotics on Minimal Hepatic Encephalopathy
Authors and Disclosures
Posted: 05/11/2011; Alimentary Pharmacology & Therapeutics. 2011;33(6):662-671. © 2011 Blackwell Publishing
Background
Minimal hepatic encephalopathy (MHE) is characterised by subtle neurocognitive deficits without overt clinical manifestations. Although several trials have individually evaluated the role of prebiotics, probiotics and synbiotics, there is yet no consensus on the management of MHE.
Aim
Aim
To estimate the efficacy of prebiotics, probiotics and synbiotics in MHE in randomised controlled trials.
Methods
Methods
MEDLINE, EMBASE, CINAHL and the Cochrane Database of Systematic Reviews were searched for published studies in all languages. Inclusion and exclusion criteria were defined a priori. Pooled relative risk and heterogeneity were estimated as the measures of association.
Results
Results
Nine studies met our inclusion criteria. Use of prebiotics, probiotics and synbiotics significantly reduced the pooled relative risk (RR) of no improvement of MHE (RR 0.40, 95% CI 0.32–0.50; P < 0.001). Upon subgroup analysis, five studies with lactulose showed significant reduction of risk of no improvement of MHE (RR 0.34, 95% CI 0.24–0.47; P < 0.0001) with no inter-trial heterogeneity. In two trials each of probiotics and synbiotics, their use was associated with significant beneficial effects (RR 0.41, 95% CI 0.26–0.65; P < 0.0001 and RR of 0.51, 95% CI 0.32–0.80; P = 0.004 respectively). There were no major adverse events though probiotics and synbiotics were better tolerated than lactulose.
Conclusions The use of prebiotics, probiotics and synbiotics was associated with significant improvement in minimal hepatic encephalopathy. Among individual agents, lactulose appears to have the most beneficial effect, followed closely by probiotics and synbiotics.
Introduction
Conclusions The use of prebiotics, probiotics and synbiotics was associated with significant improvement in minimal hepatic encephalopathy. Among individual agents, lactulose appears to have the most beneficial effect, followed closely by probiotics and synbiotics.
Introduction
Rikkers et al. first described subclinical hepatic encephalopathy in cirrhotic patients who by conventional neurological and mental status examination appeared normal but had abnormalities in psychometric tests.[1] Now recognised as Minimal Hepatic Encephalopathy (MHE),[2] it is a part of spectrum along hepatic encephalopathy characterised by abnormalities in psychometric and neurophysiological tests without overt clinical symptoms.[3–5] Incidence of MHE ranges from 30 to 84% in patients with chronic liver disease.[3] MHE is an under diagnosed problem, but its effect on daily activities could be profound as it impairs attention span and reaction time.[6] Wein et al. showed that MHE impairs fitness to drive.[2] Similar observations by Bajaj et al. in this subpopulation of cirrhotics confirm that MHE is a strong predictor for traffic violations and accidents.[3,7] Cirrhotics with MHE have poor health related quality of life[5] and impaired daily functioning as confirmed by lower scores on the sickness impact profile (SIP).[8] MHE impairs employability; up to 60% of blue collar workers and 23% of white collar workers maybe unfit for working.[9]
The major treatment modalities for MHE have been similar to that of overt hepatic encephalopathy (OHE): targeting ammonia production and absorption. As the gut microbiota play an important role in the generation of ammonia, its modulation using prebiotics, probiotics and synbiotics have been evaluated by several small studies as a therapeutic option for MHE. Prebiotics are defined as a nondigestible food ingredient that beneficially affects the host by selectively stimulating the growth and/or activity of one or a limited number of bacteria in the colon, and thus improves host health.[10] Probiotics are 'live microbial feed supplement which beneficially affects the host animal by improving its intestinal microbial balance'.[11] The combination of prebiotics and probiotics is known as a synbiotic.
The studies using these agents (prebiotics probiotics and synbiotics) have been conducted in a small number of patients with short treatment duration. As a result of seemingly inadequate data, patients with MHE often go untreated, thus potentially subjecting them to all its complications. Pooled results of the available trials would give more conclusive and stronger evidence about the role of gut based therapy. Hence, we conducted a meta-analysis of available randomised controlled trials (RCT) to further ascertain the effect of prebiotics probiotics and synbiotics and resulting gut flora modulation on course of MHE. As MHE remains undertreated, evaluating the efficacy of the available treatment options is of critical importance.Methods
Literature Search
Two independent reviewers (SS, AS) searched MEDLINE, EMBASE, CINAHL and the Cochrane Database of Systematic Reviews and Cochrane Controlled Trials Register. The search was restricted to human studies in adult subjects from January 1966 to June 2010. The search terms used were 'minimal hepatic encephalopathy', 'subclinical hepatic encephalopathy', 'latent hepatic encephalopathy''probiotics', 'prebiotics', 'synbiotics', 'lactulose', 'lactitol', 'fibre''gut flora' and 'cirrhosis'. The abstracts of all the studies were reviewed and most of the times full text reports were evaluated. The search was extended by review of bibliography of the pertinent retrieved clinical trials and other papers on the subject without language restriction. The authors were contacted when the methodology of the clinical trial or the result was not clear or relevant data not reported.
Selection
Inclusion criteria were: (i) studies involving patients with MHE or subclinical hepatic encephalopathy (SHE), (ii) study had to be a RCT comparing use of prebiotics, probiotics or synbiotics with a placebo, (iii) patients 18 years or older with established cirrhosis irrespective of the aetiology, and (iv) the study should have reported clinical outcome with regard to reversal, maintenance of MHE or worsening to OHE. The exclusion criteria were: (i) studies involving patients with OHE at the onset of clinical trial, (ii) nonrandomised controlled trial, (iii) any coexistent psychiatric illness, (iv) use of psychotropic drugs or presence of active alcoholism in patients, and (v) use of antibiotics including rifaximin or neomycin. The primary outcome evaluated was any change in the course of MHE with treatment as reported by individual clinical trials. The secondary outcome was the effect of treatment on changes in venous ammonia levels and adverse events specific to use of the drugs.
Data Abstraction
The review process was carried out as per the guidelines laid by the QUOROM statement.[12] The reviewers independently assessed the eligibility of each study for inclusion. Non-English studies that fit the inclusion criteria were translated. Any discrepancy in the selection of studies or data retrieved by the reviewers was resolved by discussion with a third reviewer. The following data from the included trials was recorded: inclusion and exclusion criteria, aetiology and method of diagnosis of cirrhosis, method used to diagnose MHE, agent and duration of treatment, side effect profile, and changes in serum ammonia levels when available. We recorded the course of MHE as reported by individual studies, based on their own criteria of diagnosing and following up MHE. The methodological quality of the included trials was assessed using the Jadad 5 point scoring system. This scale evaluates an RCT via three itemised scoring system: randomisation (0–2 points), masking (0–2 points) and dropouts and withdrawals (0–1 point), with a score of 3 considered acceptable and a higher score indicating better reporting.[13] Each study was given a total score with a maximum of five.
Data Analysis
Data Analysis
The effect of gut flora altering regimens on the neuropsychological changes of MHE was evaluated in three different ways. The primary analysis focused on evaluating the effect of combined medical therapy involving prebiotics probiotics and synbiotics on the course of MHE. Further subgroup analysis was performed to evaluate the effect of these agents individually. Next, effect of treatment regimen on serum ammonia levels and any adverse effect were evaluated. We measured weighted κ to assess interrater variability for study inclusion and assessment of the methodological quality. From each study outcome, the risk ratio (RR) with 95% CI was derived. The results were pooled using the Mantel-Haenszel (M-H) fixed effects model and the random effects model was to be used for outcomes if heterogeneity was present. With the M-H model, based on number of patients that had no worsening of MHE, weighting for each study was calculated to form an average overall outcome statistic and 95% CI. Both χ2 and I 2 statistics were analysed to assess heterogeneity between the studies. Using the χ2, a P value less than 0.1 was considered significant heterogeneity and using the I 2 statistics, 0% to 40% unimportant, 30% to 60% moderate, 50% to 90% substantial and 75% to 100% considerable heterogeneity.[14] All statistical analysis was performed using stata software version 10.0 (StataCorp, College Station, TX, USA)
Results
Results
Our search yielded a total of 174 potential articles, of which 165 were excluded (Figure 1). Nine RCT's with a total of 349 patients met our specified criteria.[15–23] Of these, five evaluated the effect of lactulose,[19–23] two of synbiotics[15,16] and two of probiotics[17,18] on MHE. Eight potentially relevant trials were identified which used lactitol, however, they were excluded either because comparison was not with a placebo, but with an antibiotic[24,25] or different doses of lactitol,[26] or lactulose[27–31] or included patients with OHE.[31] Four controlled trials with lactulose were excluded because either they did not report the outcome of interest (number of patients that improved or worsened with treatment[32] but only mean change in the psychometric tests) or involved patients with OHE[33] or were not placebo controlled (compared with fructo-oligosaccharides[34]) or was not an RCT.[35] Similarly, search with fibre yielded a study with acarbose[36] in low grade hepatic encephalopathy that was excluded from our review as it did not report the outcomes of interest.

| Figure 1. Flowchart of selection of trials. |
The term latent hepatic encephalopathy yielded several studies none of which met our inclusion criteria i.e. either were not a RCT or did not study the agents of interest in the treatment. We contacted two primary authors[16,18] and received the information about the results of trial outcomes from both the authors. While five studies used the term MHE,[15–18,21] four reported their patient population to have SHE.[19,20,22,23] As the patients in the group with SHE did not have overt hepatic encephalopathy and SHE is now synonymous with MHE, they were included in our analysis. The interrater agreement between the study reviewers for study inclusion was excellent with κ = 0.92.
Table 1 shows the design and the characteristics of the trials. Briefly, the trials were similar with respect to the patient population studied. The age group of patients included was homogeneous ranging from 44 to 62 in the treatment group and 45 to 65 in the placebo group. Males formed the predominant patient population in four studies.[15,21–23] All the studies enrolled patients diagnosed with cirrhosis of different aetiology including alcohol, viral, autoimmune, except one[17] which described its patient population as non-alcoholic cirrhotics. The method of diagnosis of cirrhosis in the patients was described by all the studies except one.[17] Furthermore, all but one study[19] reported CPT scoring of the patients at the onset of the trial. The trial durations ranged from 15 days to 6 months.
All studies used abnormality in neuropsychometric tests (outside the mean ± 2 s.d.) for the diagnosis (except for the study by Horsmans et al. [19]) and response to treatment of MHE (Table 2). The neuropsychometric tests used in the studies were different (Table 2). Three studies used abnormality in one test,[15–18] while others used two or more abnormal tests to diagnose and report outcomes of MHE.[20–23] In the study by Horsmans et al.,[19] the patients involved cirrhotics with documented portosystemic shunting without overt encephalopathy. These patients had abnormalities in neuropsychometric tests at baseline, although these tests were not formally used to divide the patients into MHE and non-MHE groups. Table 2 shows the type and doses of the agents used in respective trials. The studies differed in terms of the treatment regimen utilised to alter the gut flora. While two studies used synbiotic preparation,[15,16] two used probiotics[17,18] and five studies used lactulose (a prebiotic).[19–23]
The quality of the studies included in our analysis was good except for one[18] which had a Jadad score of 2. Six of the studies[15,17,20–23] had a score of three, while the remaining two had a score four[19] and five.[16] The mean Jadad score of all the trials included in our study was 3.22.
The alteration of gut flora using pre, pro and synbiotic significantly reduced the risk of no improvement of MHE compared with placebo (RR 0.40, 95% CI 0.32–0.50; P < 0.001; Figure 2, nine trials). There was no significant heterogeneity between the trials (χ2 = 10.22, P = 0.250, I 2 = 22%). A post hoc subgroup analysis of this data excluding the study with a low Jadad score[18] revealed similar results (RR 0.39, 95% CI 0.31–0.50; P < 0.001; Figure S1, eight trials) with no significant intertrial heterogeneity (χ2 = 10.36, P = 0.169, I 2 = 32%).
Click Figure To Enlarge;

Figure 2.
Number of patients without improvement of MHE in trials with prebiotics, probiotics and synbiotics compared with control (fixed effects analysis). CI, confidence interval; RR, relative riskFive studies provided data on change in course of MHE with lactulose. Using the Mantel-Haenszel model, the use of lactulose significantly reduced the risk of no improvement of MHE in comparison with placebo (RR of 0.34, 95% CI 0.24–0.47; P < 0.0001; Figure 3). There was no significant heterogeneity between the studies (χ2 = 6.11, P = 0.191, I 2 = 35%). Furthermore, two studies with synbiotics too showed that their use reduced the risk of no improvement of MHE (RR 0.51, 95% CI 0.32–0.80, P = 0.004; Figure 4) with no significant intertrial heterogeneity (χ2 = 0.74, P = 0.390, I 2 = 0%). Similar results were obtained with two studies using probiotics i.e. reduced risk of no improvement of MHE with RR 0.41 (95% CI 0.26–0.65, P < 0.0001; Figure 4) without heterogeneity with χ2 = 0.65, P = 0.421, I 2 = 0%. Venous ammonia levels were evaluated by four studies, two of which used synbiotics,[15,16] one probiotic[17] and another with lactulose.[23] The pooled results showed that therapy led to lowering of serum ammonia in these patients (WMD −19.85, 95% CI −22.94 to −16.77, P < 0.0001 with some heterogeneity among the studies with χ2 = 5.73, P < 0.125, I 2 = 48%.
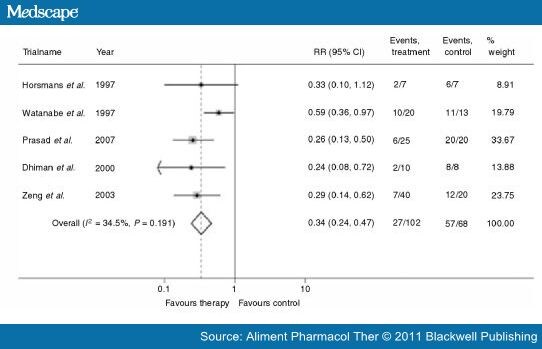
Figure 3.
Number of patients without improvement of MHE in trials with Lactulose compared with control (fixed effects analysis). CI, confidence interval; RR, relative risk.

Figure 4
Number of patients without improvement of MHE in trials with synbiotics and probiotics compared with control (fixed effects analysis). CI, confidence interval; RR, relative risk.
Of the four studies that evaluated the use of probiotics and synbiotics, three[15–17] contained information about adverse effects. These were mainly confined to gastrointestinal system and the study by Malaguarnera et al. included abdominal pain, nausea in the treatment group and diarrhea, headache in the placebo group. In the study by Bajaj et al. two patients dropped out because they did not like the taste of the probiotic. The study by Liu et al. reported good tolerance of the agents in all patients with no adverse effects. Overall, none of these studies reported any serious adverse effects in the patients. In the five studies evaluating the effect of lactulose, two studies[19,20] reported adverse effects. In the study by Horsman et al. three patients reported diarrhoea with the use of lactulose that required dose reduction. In the study by Watanabe et al. eight patients (19%) reported diarrhoea, one reported soft stools, one anorexia, one abdominal pain, one vomiting, one glycosuria (out of the total 43 patients who received lactulose in this study). None reported any serious adverse effect that required withdrawal from the study. As most of the studies did not reliably give information about the adverse effects in the respective treatment and the placebo group, we were unable to perform a meta-analysis of this outcome.
Number of patients without improvement of MHE in trials with synbiotics and probiotics compared with control (fixed effects analysis). CI, confidence interval; RR, relative risk.
Of the four studies that evaluated the use of probiotics and synbiotics, three[15–17] contained information about adverse effects. These were mainly confined to gastrointestinal system and the study by Malaguarnera et al. included abdominal pain, nausea in the treatment group and diarrhea, headache in the placebo group. In the study by Bajaj et al. two patients dropped out because they did not like the taste of the probiotic. The study by Liu et al. reported good tolerance of the agents in all patients with no adverse effects. Overall, none of these studies reported any serious adverse effects in the patients. In the five studies evaluating the effect of lactulose, two studies[19,20] reported adverse effects. In the study by Horsman et al. three patients reported diarrhoea with the use of lactulose that required dose reduction. In the study by Watanabe et al. eight patients (19%) reported diarrhoea, one reported soft stools, one anorexia, one abdominal pain, one vomiting, one glycosuria (out of the total 43 patients who received lactulose in this study). None reported any serious adverse effect that required withdrawal from the study. As most of the studies did not reliably give information about the adverse effects in the respective treatment and the placebo group, we were unable to perform a meta-analysis of this outcome.
Discussion
While the natural history of MHE remains to be completely elucidated, it is known that it may progress to OHE[4,37,38] and may have a fluctuating course. As the neurocognitive deficits seen in MHE impair driving skills and other important aspects such as ability to work, early recognition and treatment of this condition is warranted. Once MHE has been diagnosed it can be challenging for the physician to decide which agent would be the most effective in reversing the neurocognitive deficits. Several different treatment options exist but there is yet no definite standard of care mainly because of the variable efficacy and side effect profile of the available options. A recently published editorial underscored the importance of studies that elucidate the effect of changing gut flora composition (using pre and probiotics) for the treatment of hepatic encephalopathy.[39] The results of our pooled analysis provide significant evidence that bridges the knowledge gap of MHE, thus providing an impetus for treatment.
Modulation of gut flora presumably works by several mechanisms in cirrhosis to exert a favourable effect on neurological dysfunction.[40] As reported by Liu et al. [15] and Lata et al. [18] the reduction in potential pathogenic bacteria such as Escherichia coli and Staphylococcal species in stool at the end of treatment period with increase in non-urease producing Lactobacillus limits ammonia production. Moreover, lactulose is converted to lactic and acetic acid which results in acidification of colonic contents. The low pH decreases passive non-ionic diffusion of ammonia thus lowering its systemic concentration. Furthermore, with its prebiotic potential, lactulose also encourages growth of probiotic bacteria such as Bifidobacterium species that are known to have health-promoting effects. While this potential therapeutic target of modifying the gut microbiota using pre–pro or synbiotics has been evaluated in other conditions such as inflammatory bowel disease,[41] irritable bowel syndrome,[42,43] antibiotic-associated diarrhoea,[44,45] to our knowledge this is the first meta-analysis to assess the beneficial effect of these agents in MHE.
The results in our study are reported using the fixed-effects model and showed a lack of any inter-trial heterogeneity, thus strengthening the outcomes. Moreover, all studies were conducted in patients with documented cirrhosis and not a reversible hepatic dysfunction such as alcoholic or viral hepatitis. Furthermore, the studies had a mixture of patients with CPT scoring in all categories (except one study[17]) with consistent relative risk reduction among all, pointing towards the usefulness of treatment irrespective of the initial CPT scoring of the patients. The presence of MHE in the study subjects or worsening to OHE during follow-up was not resulting from any confounding insult to the liver such as intercurrent infections, concomitant alcohol use or any other illness that could worsen hepatic function. This along with the short duration of the study periods and with a consistent beneficial effect in each trial further strengthen the evidence that the therapeutic action in MHE can be ascribed to the use of the individual agents themselves and not to a chance finding.
Although patients in the studies with lactulose did report problems related to palatability, diarrhoea and flatulence, overall it was well tolerated as all studies titrated the dose to two to three bowel movements per day. The patient acceptability of probiotics or synbiotics seemed better with no reported adverse effect except for issue with palatability of the probiotic in the study by Bajaj et al. which again could be ascribed to the specific manufacturer of the probiotic (flavoured vs. unflavoured). As the agent in this study was not strictly a probiotic but yogurt, any beneficial as well as adverse effect could also be ascribed to its other constituents including lactose and milk protein. Although the trials individually showed significant reduction in venous ammonia levels, the results of our pooled analysis showed some heterogeneity. A wide variance in the mean serum ammonia levels in the studies along with small population size could be possible contributors to this effect. Based on this we conclude that the reduction in venous ammonia levels should be interpreted with caution.Our meta-analysis has several limitations, related both to our study and to the inherent nature of meta-analyses. The result of any meta-analysis depends upon the quality of the RCT's included. Hence the result of our study is limited because of the nature of the trials included. Firstly, the duration of all the included trials is short. While this could be appropriate in patients with OHE who may have a dramatic clinical presentation which changes with treatment or sometimes spontaneously after the precipitating event is corrected, patients with MHE have a more subtle course. A trial over a longer duration would give a better picture of the extent of benefit effect. Second, the number of patients included in each trial is small. While a meta-analysis mathematically combines these patients to develop overall picture, a small number of included patients do increase the alpha error that would be associated with the study. Next, the difficulty with any study with hepatic encephalopathy and especially with MHE is a lack of a standard diagnostic test. The International Society for Hepatic Encephalopathy and Nitrogen metabolism (ISHEN committee) itself acknowledges the current lack of consensus on how best to detect MHE.[46] To the extent that neuropsychological tests have more face validity as they directly measure cognitive functions, the PSE-Syndrome test is a battery recommended for assessment for MHE by the committee. Most of the studies included in this meta-analysis used tests which are components of the PSE-Syndrome-test. Meta-analyses tend to have shortcoming of their own. In general, data retrieved from a well conducted, adequately powered randomised controlled trial cannot be replaced by a meta-analysis. However, to design a study in MHE addressing the limitations cited above and appropriately evaluate the effect of treatment would require a large, well conducted trial over a more prolonged period. Until that is done, the results from a well conducted meta-analysis would be of considerable importance to shed some light on this newly evolving area of considerable importance. Furthermore, we attempted to minimise publication bias in our study by conducting a comprehensive literature search. Additionally, as the studies included in our analysis also contained negative and nonsignificant end results, our study is less likely to be affected by negative publication bias. Evaluation for heterogeneity in outcomes is another factor that requires consideration while interpreting meta-analyses. The results of our study, however, showed that there was a very minor heterogeneity across the studies.
Our findings have important implications for the clinical practice as well as research in relation to MHE. The results of our study provide the strongest yet available evidence for the use of prebiotics, probiotics and synbiotics in management of MHE. Furthermore, we conclude that while each of the agents individually have a role, lactulose appears to be the most studied and beneficial followed closely by probiotics and synbiotics. Probiotics may be particularly useful in scenarios of noncompliance or intolerance to lactulose. Moreover, the beneficial effect of these agents with a relatively low side effect profile further necessitates the need for recognising and treating MHE. Whether or not treatment of MHE has any mortality benefits over a longer period of time needs to be addressed in large-scale clinical trials.
No comments:
Post a Comment