Christoph Sarrazin,
Stefan Zeuzem
Article first published online: 4 JAN 2011
DOI: 10.1111/j.1478-3231.2010.02398.x
Abstract
Approximately 180 million individuals (i.e. 2.5% of the world population) are estimated to have chronic hepatitis C virus (HCV) infection, with the highest prevalence reported in Egypt and the lowest in Finland (1, 2). HCV belongs to the Flaviviridae family and is a small 55 nm virus with a lipid envelope and a single-stranded RNA viral genome with approximately 9600 nucleotides (3, 4). The positive-strand RNA genome includes a 5′-non-coding region with an internal ribosome entry site, an open reading frame that encodes structural (core, envelope 1, 2, p7) and non-structural (NS2, NS3, NS4A, NS4B, NS5A, NS5B) proteins and a 3′-non-coding region. The internal ribosome entry site causes the translation of a polyprotein precursor, which is processed into mature structural and non-structural proteins (5).
The most common screening test for HCV is an immunoassay [enzyme immunoassay (EIA), microparticle EIA, chemiluminescence immunoassay (CIA)] that detects anti-HCV antibodies. These assays have many advantages for diagnosis: they are easy to use, automation is simple, have a low variability and are inexpensive.
Nowadays, the detection of antibodies directed against various HCV epitopes in plasma or serum is based on the use of third-generation EIAs. These assays detect antibodies to recombinant antigens from core (c22) and non-structural proteins 3 (c33), 4 (c100, c200) and 5. The specificity and sensitivity of third-generation immunoassays in patients with chronic liver disease were found to be >98 and >97% respectively (15–17). The mean time to seroconversion is shortened by 2–3 weeks with third-generation compared with second-generation assays with the detection of HCV-specific antibodies approximately 4–6 weeks after infection (18). Anti-HCV-IgM detection cannot discriminate between acute and chronic hepatitis C because some chronically infected patients produce anti-HCV IgM intermittently and not all patients respond to acute HCV infection by producing anti-HCV IgM. Anti-HCV antibodies may become undetectable via commercial assays in some patients many years after successful treatment.
Detection and quantification of hepatitis C virus RNA
There are a number of different commercial assays approved by the FDA and EMEA for the determination of HCV RNA (19–24).
Cobas® Amplicor HCV version 2.0 (Roche Molecular Diagnostics, Pleasonton, CA, USA) based on a standard reverse transcription-polymerase chain reaction (RT-PCR) is available for the qualitative measurement of HCV RNA. The lowest detection limit is 50 IU/ml whatever the HCV genotype (19).
The versant HCV quantitative Test (Siemens Healthcare Diagnostics) is a quantitative HCV RNA assay based on signal amplification by branched DNA (bDNA). The bDNA assay version 3.0 is standardized for IU, and the assay has been reported to be linear over its entire dynamic range from the lower detection limit of 615 IU/ml to 8 million IU/ml whatever the HCV genotype (22).
The COBAS® Amplicor HCV Monitor 2.0 (CAM, Roche Molecular Diagnostics) is a standard RT-PCR-based assay with a linear detection range of 500–500 000 IU/ml, whatever the HCV genotype. For higher HCV RNA concentrations, predilution of the original sample is required (21).
Currently, two real-time PCR assays are available: the COBAS® Ampliprep/Cobas® TaqMan® assay (CAP/CTM, Roche Molecular Diagnostics) and the real-time HCV assay (also named AccuGene® HCV, Abbott Molecular Inc., Des Plaines, IL, USA). These assays have the advantage of having a broad dynamic range of amplification, thus improving the limits of detection (LOD) to ≤10 IU/ml, and linear quantification up to 107–108 IU/ml (26, 27).
The results of the Roche CAP/CTM are reported in four stages: (a) undetectable (below the detection limit), (b) positive but unquantifiable (less then 15 IU/ml), (c) detectable and quantifiable (more then 15 IU/ml), reported as an exact HCV RNA concentration in IU/ml above 30–40 IU/ml, or (d) detectable, quantifiable but above the upper limit (more then 6.9 × 107 IU/ml) (28, 29).
It has also been shown that the results of assays can vary significantly with different HCV genotypes despite IU standardization. Generally, the HCV RNA levels in genotype 1 samples measured with the Roche CAP/CTM are higher than those obtained by the Abbott real-time HCV assay and the Siemens bDNA assay (approximately 0.5 log10 IU/ml), while the HCV RNA concentrations in samples with genotype 4 are lower (26, 29–31).
The determination of HCV subtypes has no clinical relevance for the current standard of care with pegylated IFN/ribavirin therapy, while different treatment durations based on viral kinetics are recommended based on different HCV genotypes.
Novel, direct-acting antiviral agents (DAA), also called ‘specifically targeted antiviral therapy for hepatitis C’, are currently under clinical development and are substantially improving the SVR rates in genotype 1 patients (40). Subtype determination may become important in future clinical practice mainly because of resistance profiles for these DAA agents according to HCV genotype and subtype. The correct identification of HCV subtypes 1a and 1b has been reported in >96% of cases for second-generation INNO-LiPA assays (41).
The diagnosis of acute HCV infection can be difficult. Although the most reliable approach is proof of seroconversion to HCV antibodies in a previously seronegative individual (42), this is rarely possible in clinical practice. The absence of detectable HCV antibodies in the acute phase does not exclude acute hepatitis C, because the appearance of antibodies can be delayed in as many as 30% of patients at the onset of symptoms (43). An impaired ability to develop antibodies is especially seen in immunocompromised patients. HCV RNA is typically detected in a seronegative patient, followed by the development of HCV antibodies several days or weeks later.
With the current standard therapy of 24–48 weeks of treatment with PEG-IFN- and ribavirin, the SVR rates are still unsatisfactory and only reach about 40–50% (12–14). In recent years, treatment regimens have been individualized in an attempt to improve the treatment response with the identification of several viral- and host-related factors that affect response to antiviral therapy. Monitoring HCV RNA was found to be a key parameter in the management of response-guided therapy of chronic hepatitis C with PEG-IFN plus ribavirin.
The treatment recommendations of the current German/Austrian/Swiss guidelines are described below (46).
Treatment can also be discontinued in patients with detectable HCV RNA (more the 50 IU/ml) after 24 weeks of therapy. Once again, the chances of an SVR in these patients are minimal (1–3%) (12, 48, 52).
Because of the higher sensitivity of the current most extensively used real-time PCR-based HCV RNA assays (LOD less then 10 IU/ml) and with the extension of therapy to up to 72 weeks, the negative predictive value (NPV) of the 2 log rule and the stopping rule at week 24 based on HCV RNA detectability must be re-evaluated. In the INDIV-2 study, for example, patients with initial HCV RNA negativity by a highly sensitive assay at week 30 were treated for 72 weeks and achieved SVR rates of 50% (53).
Low-dose monotherapy with PEG-IFN- in patients who fail to respond to a full course of antiviral therapy cannot be recommended. Three independent studies did not show a significant improvement in histological and/or clinical courses in these patients. Whether certain sub-groups (i.e. patients with portal hypertension) can benefit from low-dose PEG-IFN monotherapy remains to be determined (54–56).
Treatment duration for genotype 1(4)-infected patients
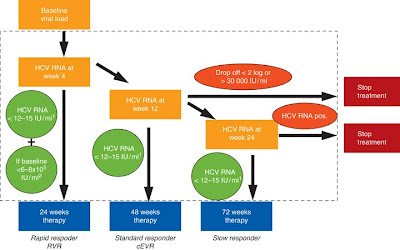
Twenty-four weeks of treatment is recommended for genotype 1 patients with a low baseline viral load (VL) (less then 600 000–800 000 IU/ml) who achieve a rapid virological response (RVR; HCV RNA less then 50 IU/ml at week 4 of treatment). There was no significant difference in the SVR rates when patients with RVR and low VL were treated for 24 weeks or 48 weeks (57–59) (Fig. 1). There are few data on a reduced treatment duration in patients with advanced fibrosis, steatosis and insulin resistance, and thus shortened treatment should not be considered for these groups (60–62).
Various studies have investigated the benefit of extending treatment in genotype 1-infected slow responders [patients with detectable (≥50 IU/ml) HCV RNA levels at week 12, but undetectable HCV RNA at week 24] (50, 52, 63–66)
Various studies have investigated the benefit of extending treatment in genotype 1-infected slow responders [patients with detectable (more then 50 IU/ml) HCV RNA levels at week 12, but undetectable HCV RNA at week 24] (50, 52, 63–66) (Table 1). Analysis of three different European studies showed significantly higher SVR and lower relapse rates in the 72-week compared with the 48-week treatment group (52) (Fig. 1).
(Table 1).

Patients who attain a complete early virological response (cEVR; undetectable HCV RNA at week 12 using an assay with a lower limit of quantification cut-off of 50 IU/ml) should be treated for 48 weeks (50, 52, 64, 65) (Fig. 1).
Currently, baseline VL is only used to shorten the treatment duration in rapid responders. However, the determination of low and high baseline VL may also be useful in patients with cEVR. Higher SVR rates were reported in patients with high baseline viraemia and cEVR if therapy was prolonged to 60–72 weeks (53, 64).
Various studies have investigated the reduction of treatment to 12–16 weeks. Overall, reducing the treatment to less then 24 weeks increases the number of relapsers. However, many HCV genotype 2/3 patients may be treated for 12–16 weeks if certain preconditions are fulfilled, especially an RVR because only patients with RVR at week 4 had high SVR rates after 16, 14 or even 12 weeks of treatment (67–72) (Table 2). Nevertheless, in the ACCELERATE study, patients who received PEG-IFN-2a (180 μg/week) plus a fixed ribavirin dose of 800 mg per day achieved significantly lower SVR rates with a shorter treatment (79 vs 85%) (67).
Table 2. Shortening the treatment to 12–16 weeks in genotype 2/3-infected rapid responders (46)
Click To Englarge

In addition to RVR, the specific HCV genotype and the baseline VL are associated with a virological response. HCV genotype 2 patients respond better to pegylated IFN and ribavirin than those infected with genotype 3 (61).
Furthermore, patients with a low baseline VL (less the 400 more then 400 000–800 000 IU/ml) (67, 69).
Genotype 2/3-infected patients with a baseline VL less then 400 000–800 000 IU/ml and RVR can be considered for a shorter treatment. Ribavirin dosing appears to be an important factor in defining the treatment outcome: shorter treatment durations have mainly been effective in studies with a weight-based ribavirin regimen, whereas studies with a fixed ribavirin dose of 800 mg per day have generally resulted in a significant decrease in SVR with a shorter treatment. However, reducing the duration of treatment is not recommended in patients with advanced liver fibrosis or those with low alanine transaminase values at baseline (67, 70, 74).
Genotype 2/3-infected patients who do not achieve RVR showed low SVR rates (45–55%)(67, 72, 75). Whether patients without an RVR should be treated for longer than 24 weeks is based on retrospective studies. These data show that genotype 2/3-infected patients without an RVR who receive 48 weeks of PEG-IFN-2a plus ribavirin 1000/1200 mg/day have higher SVR rates than those receiving 24 weeks of PEG-IFN-2a plus ribavirin 800 mg/day (76 vs 67%; relapse: 4 vs 26%) (76). Prospective studies have begun to investigate extending the treatment to 36 or 48 weeks in non-RVR patients (Fig. 2).
Figure 2. Treatment algorithm for genotype 2/3-infected patients (46). 1. Sensitive HCV RNA assays (limit of detection 12–15 or 50 IU/ml) at weeks 4 and 12 may determine the treatment duration. 2. Shorter treatment regimens are not approved. Shortening the treatment is not recommended in patients with advanced fibrosis/cirrhosis. Negative predictive factors such as hepatic steatosis and low alanine transaminase values at baseline should be considered. There are no data for patients with normal transaminases at baseline. 3. Treatment can be discontinued in all patients with detectable HCV RNA (more then 12–15 IU/ml) after 24 weeks of therapy. 4. The treatment duration (36, 48 or 72 weeks) for slow responders is not established. Prospective studies have been initiated to investigate treatment extension. HCV, hepatitis C virus.
Does the use of highly sensitive assays affect recent recommendations for a response-guided therapy?
Recommendations for the duration of treatment and early discontinuation were established using HCV RNA assays with a detection limit of less then 50 IU/ml. Numerous studies have shown that patients with a low baseline VL (less then 400 000–800 000 IU/ml) and a RVR, defined by undetectable HCV RNA at week 4, are appropriate candidates for shorter treatment regimens (12–16 and 24 weeks in genotype 2/3- and 1-infected patients respectively).
As mentioned above, the currently used real-time PCR-based CAP–CTM test has a detection limit of ≤15 IU/ml. Sarrazin and colleagues re-analysed frozen serum samples with CAP–CTM from patients with chronic hepatitis C enrolled in two large, randomized studies. The RVR rates were highly concordant for the CAM, with a LOD of 50 IU/ml, and the CAP–CTM. Although a significantly smaller number of samples had undetectable HCV RNA with the CAP–CTM, there was no difference in the SVR rates after shorter therapy in patients with an RVR less then 50 IU/ml, an RVR less then 15 IU/ml and undetectable RVR (82, 83 and 83% for 24 weeks for genotype 1 and 95, 95 and 94% for 16 weeks genotype 2/3) (77). Treatment regimens can therefore be shortened to 16/24 weeks on the basis of an RVR with HCV RNA concentrations less then 15 IU/ml by the CAP–CTM.
Genotype 1-infected patients with residual viraemia at week 12 (less then 15 IU/ml, but detectable by CAP–CTM) have also been shown to have a high relapse rate (55%). This group may benefit from prolonged treatment (72 weeks). Furthermore, low viraemia (between 15 and 50 IU/ml) at week 12 in genotype 1-infected patients was associated with even higher relapse rates (75%) (77).
Is the time point a relevant predictor of sustained virological response?
Up-to-date virological response profiles at weeks 4 and 12 provide a robust framework for predicting SVR in patients with genotype 1 infection. Neumann and colleagues investigated the positive predictive value (PPV) and NPV of an EVR at weeks 2 and 4 during treatment with IFN-2b or pegylated IFN-2a in treatment-naïve patients infected with genotype 1. All patients with undetectable HCV RNA at week 2 achieved an SVR (PPV: 100%). Patients with a rapid initial virological response at week 2, defined as an HCV RNA decline more then 2 log10IU/ml, had a high PPV for SVR of 88–97%. A VL more the 6 log10 IU/ml at week 2 has a high NPV (82–100%) for achieving an SVR. The combination of VL and viral decline (VD) at week 4 had the best NPV. A VL more then 5.5 log10 IU/ml and VD less then 2 log10 IU/ml had a 100% NPV in all treatment arms (4–13% of all patients; specificity: 12–29%) (78).
Conclusion
Despite an improvement in anti-HCV therapy in the last few years, the treatment of chronic hepatitis C is still challenging and must be improved. Many viral-related factors have been evaluated in association with the virological response to PEG-IFN- and ribavirin-based therapy. It is currently agreed that the algorithms for treatment duration and early discontinuation can be applied based on highly sensitive HCV RNA assays (LOD≤15 IU/ml) (77, 79).
One of the most important patient predictors of a reduced SVR rate is advanced fibrosis and cirrhosis. Other patient-related factors negatively influencing the treatment outcome are ethnicity, male gender, older age, higher body weight, liver steatosis, elevated pretreatment serum -glutamyltransferase levels and the recently identified polymorphism upstream from IL-28B (rs12979860) (80–82).
Several independent genome-wide association studies have reported the presence of single nucleotide polymorphisms in the IL28B region to be associated with response to treatment (83, 84). The exact mechanisms underlying this association between IL28B polymorphism and response to treatment are unknown (85).
The gene IL-28B on chromosome 19 codes for IFN-λ-3. The protein product is one of the three members of the recently described type 3 IFN family (86). In Caucasians infected with genotype 1, the CC IL-28B type was associated with improved early viral kinetics and a greater likelihood of RVR (28 vs 5 vs 5% for CC, CT, TT respectively) and cEVR (87 vs 38 vs 28%) and SVR (69 vs 33 vs 37%) (82). Recently, it was shown that the IL28B polymorphism (rs12979860) also determines the treatment response in genotype 2- or 3-infected patients who do not achieve RVR (87).
In the future, DAA such as the protease inhibitors telaprevir and boceprevir in addition to PEG-IFN- and ribavirin will improve the SVR rates in treatment-naïve genotype 1 patients as well as in genotype 1-infected non-responders and relapsers to standard therapy. Clinical trials with the NS3/4A protease inhibitor telaprevir show that the treatment duration can be shortened to 24 weeks in more than 60% of patients (40). The results from on-treatment HCV RNA measurements must be analysed and response-guided algorithms must be established based on the correlation of baseline VL with RVR and SVR.
Telaprevir will be approved for a 24-week course in patients with undetectable HCV RNA at weeks 4 and 12 (extended RVR). For all other patients, 48 weeks of treatment is recommended. Treatment algorithms for boceprevir will be different. After a 4-week lead-in phase of PEG-IFN- plus ribavirin, boceprevir will be added for either 24 or 48 weeks. Individuals achieving an RVR at week 8 will be treated for a total of 28 weeks, while patients showing a clearance of the virus between weeks 8 and 12 of treatment will continue for a total of 48 weeks. Sarrazin has served as a clinical investigator, consultant and/or member of speakers' bureau for Abbott, Roche and Siemens. S. Zeuzem has served as a clinical investigator, consultant and/or member of speakers' bureau for Abbott, Achillion, Anadys, BMS, Gilead, Merck, Novartis, Pfizer, Roche, Tibotec and Vertex. P. de Leuw has no conflicts to declare.
Lavanchy D. The global burden of hepatitis C. Liver Int 2009; 29 (Suppl. 1): 74–81.
Direct Link:
Abstract
Full Article (HTML)
PDF(178K)
References
2
Esteban JI, Sauleda S, Quer J. The changing epidemiology of hepatitis C virus infection in Europe. J Hepatol 2008; 48: 148–62.
CrossRef,
PubMed,
Web of Science® Times Cited: 64
3
Houghton M, Weiner A, Han J, et al. Molecular biology of the hepatitis C viruses: implications for diagnosis, development and control of viral disease. Hepatology 1991; 14: 381–8.
PubMed,
ChemPort,
Web of Science® Times Cited: 773
4
Wakita T, Pietschmann T, Kato T, et al. Production of infectious hepatitis C virus in tissue culture from a cloned viral genome. Nat Med 2005; 11: 791–6.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 759
5
Moradpour D, Penin F, Rice CM. Replication of hepatitis C virus. Nat Rev Microbiol 2007; 5: 453–63.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 190
6
Villano SA, Vlahov D, Nelson KE, et al. Persistence of viremia and the importance of long-term follow-up after acute hepatitis C infection. Hepatology 1999; 29: 908–14.
Direct Link:
Abstract
PDF(83K)
References
7
Gerlach JT, Diepolder HM, Zachoval R, et al. Acute hepatitis C: high rate of both spontaneous and treatment-induced viral clearance. Gastroenterology 2003; 125: 80–8.
PubMed,
Web of Science® Times Cited: 216
8
Orland JR, Wright TL, Cooper S. Acute hepatitis C. Hepatology 2001; 33: 321–7.
Direct Link:
Abstract
PDF(161K)
References
9
Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med 2007; 147: 677–84.
PubMed,
Web of Science® Times Cited: 83
10
Morgan TR, Ghany MG, Kim HY, et al. Outcome of sustained virological responders with histologically advanced chronic hepatitis C. Hepatology 2010; 52: 833–44.
Direct Link:
Abstract
Full Article (HTML)
PDF(583K)
References
11
Zeuzem S, Berg T, Moeller B, et al. Expert opinion on the treatment of patients with chronic hepatitis C. J Viral Hepat 2009; 16: 75–90.
Direct Link:
Abstract
Full Article (HTML)
PDF(743K)
References
12
Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet. 2001; 358: 958–65.
PubMed,
ChemPort,
Web of Science® Times Cited: 2830
13
Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002; 347: 975–82.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 2548
14
McHutchison JG, Lawitz EJ, IDEAL Study Team et al. Peginterferon alfa-2b or alfa-2a with ribavirin for treatment of hepatitis C infection. N Engl J Med 2009; 361: 580–93.
CrossRef,
ChemPort,
Web of Science® Times Cited: 85
15
Colin C, Lanoir D, HEPATITIS Group et al. Sensitivity and specificity of third-generation hepatitis C virus antibody detection assays: an analysis of the literature. J Viral Hepat 2001; 8: 87–95.
Direct Link:
Abstract
Full Article (HTML)
PDF(73K)
References
16
Sookoian S, Castaño G. Evaluation of a third generation anti-HCV assay in predicting viremia in patients with positive HCV antibodies. Ann Hepatol 2002; 1: 179–82.
17
Alborino F, Burighel A, Tiller FW, van Helden J, et al. Multicenter evaluation of a fully automated third-generation anti-HCV antibody screening test with excellent sensitivity and specificity. Med Microbiol Immunol 24 September 2010 [Epub ahead of print] DOI: DOI: 10.1007/s00430-010-0171-0.
18
Uyttendaele S, Claeys H, Mertens W, et al. Evaluation of third-generation screening and confirmatory assays for HCV antibodies. Vox Sang 1994; 66: 122–9.
Direct Link:
Abstract
PDF(746K)
References
19
Nolte FS, Fried MW, Shiffman ML, et al. Prospective multicenter clinical evaluation of AMPLICOR and COBAS AMPLICOR hepatitis C virus tests. J Clin Microbiol 2001; 39: 4005–12.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 29
20
Lee SC, Antony A, Lee N, et al. Improved version 2.0 qualitative and quantitative AMPLICOR reverse transcription-PCR tests for hepatitis C virus RNA: calibration to international units, enhanced genotype reactivity, and performance characteristics. J Clin Microbiol 2000; 38: 4171–9.
PubMed,
ChemPort,
Web of Science® Times Cited: 100
21
Gerken G, Rothaar T, Rumi MG, et al. Performance of the COBAS AMPLICOR HCV MONITOR test, version 2.0, an automated reverse transcription-PCR quantitative system for hepatitis C virus load determination. J Clin Microbiol 2000; 38: 2210–4.
PubMed,
ChemPort,
Web of Science® Times Cited: 34
22
Ross RS, Viazov S, Sarr S, et al. Quantitation of hepatitis C virus RNA by third generation branched DNA-based signal amplification assay. J Virol Methods 2002; 101: 159–68.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 36
23
Sarrazin C, Teuber G, Kokka R, et al. Detection of residual hepatitis C virus RNA by transcription-mediated amplification in patients with complete virologic response according to polymerase chain reaction-based assays. Hepatology 2000; 32: 818–23.
Direct Link:
Abstract
PDF(209K)
References
24
Leckie G, Schneider G, Abravaya K, et al. Performance attributes of the LCx HCV RNA quantitative assay. J Virol Methods 2004; 115: 207–15.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 9
25
Hendricks DA, Friesenhahn M, Tanimoto L, et al. Multicenter evaluation of the VERSANT HCV RNA qualitative assay for detection of hepatitis C virus RNA. J Clin Microbiol 2003; 41: 651–6.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 26
26
Vermehren J, Kau A, Grtner BC, et al. Differences between two real-time PCR-based hepatitis C virus (HCV) assays (RealTime HCV and Cobas AmpliPrep/Cobas TaqMan) and one signal amplification assay (Versant HCV RNA 3.0) for RNA detection and quantification. J Clin Microbiol 2008; 46: 388–91.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 12
27
Schutten M, Fries E, Burghoorn-Maas C, et al. Evaluation of the analytical performance of the new Abbott RealTime RT-PCRs for the quantitative detection of HCV and HIV-1 RNA. J Clin Virol 2007; 40: 99–104.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 12
28
Sarrazin C, Dragan A, Grtner BC, et al. Evaluation of an automated, highly sensitive, real-time PCR-based assay (COBAS Ampliprep/COBAS TaqMan) for quantification of HCV RNA. J Clin Virol 2008; 43: 162–8.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 11
29
Sizmann D, Boeck C, Boelter J, et al. Fully automated quantification of hepatitis C virus (HCV) RNA in human plasma and human serum by the COBAS AmpliPrep/COBAS TaqMan system. J Clin Virol 2007; 38: 326–33.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 27
30
Sarrazin C, Grtner BC, Sizmann D, et al. Comparison of conventional PCR with real-time PCR and branched DNA-based assays for hepatitis C virus RNA quantification and clinical significance for genotypes 1 to 5. J Clin Microbiol 2006; 44: 729–37.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 42
31
Chevaliez S, Bouvier-Alias M, Brillet R, et al. Overestimation and underestimation of hepatitis C virus RNA levels in a widely used real-time polymerase chain reaction-based method. Hepatology 2007; 46: 22–31.
Direct Link:
Abstract
Full Article (HTML)
PDF(964K)
References
32
Kolykhalov AA, Feinstone SM, Rice CM. Identification of a highly conserved sequence element at the 3′ terminus of hepatitis C virus genome RNA. J Virol 1996; 70: 3363–71.
PubMed,
ChemPort,
Web of Science® Times Cited: 259
33
Tanaka T, Kato N, Cho MJ, et al. Structure of the 3′ terminus of the hepatitis C virus genome. J Virol 1996; 70: 3307–12.
PubMed,
ChemPort,
Web of Science® Times Cited: 196
34
Simmonds P. Genetic diversity and evolution of hepatitis C virus – 15 years on. J Gen Virol 2004; 85: 3173–88.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 224
35
Simmonds P, Bukh J, Combet C, et al. Consensus proposals for a unified system of nomenclature of hepatitis C virus genotypes. Hepatology 2005; 42: 962–73.
Direct Link:
Abstract
Full Article (HTML)
PDF(276K)
References
36
Germer JJ, Vandenameele JN, Mitchell PS, et al. Automated sample preparation for the TRUGENE HIV-1 genotyping kit using the MagNA pure LC instrument. Diagn Microbiol Infect Dis 2004; 49: 59–61.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 4
37
Stuyver L, Wyseur A, van Arnhem W, et al. Second-generation line probe assay for hepatitis C virus genotyping. J Clin Microbiol 1996; 34: 2259–66.
PubMed,
ChemPort,
Web of Science® Times Cited: 185
38
Stuyver L, Wyseur A, van Arnhem W, et al. Hepatitis C virus genotyping by means of 5′-UR/core line probe assays and molecular analysis of untypeable samples. Virus Res 1995; 38: 137–57.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 109
39
Zheng X, Pang M, Chan A, et al. Direct comparison of hepatitis C virus genotypes tested by INNO-LiPA HCV II and TRUGENE HCV genotyping methods. J Clin Virol 2003; 28: 214–6.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 17
40
Lange CM, Sarrazin C, Zeuzem S. Review article: specifically targeted anti-viral therapy for hepatitis C − a new era in therapy. Aliment Pharmacol Ther 2010; 32: 14–28.
ChemPort
41
Chevaliez S, Bouvier-Alias M, Brillet R, et al. Hepatitis C virus (HCV) genotype 1 subtype identification in new HCV drug development and future clinical practice. PLoS One 2009; 4: e8209.
CrossRef,
ChemPort,
Web of Science® Times Cited: 4
42
Maheshwari A, Ray S, Thuluvath PJ. Acute hepatitis C. Lancet 2008; 372: 321–32.
CrossRef,
PubMed,
Web of Science® Times Cited: 28
43
Farci P, Alter HJ, Wong D, et al. A long-term study of hepatitis C virus replication in non-A, non-B hepatitis. N Engl J Med 1991; 325: 98–104.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 449
44
Quiroga JA, Campillo ML, Catillo I, et al. IgM antibody to hepatitis C virus in acute and chronic hepatitis C. Hepatology 1991; 14: 38–43.
Direct Link:
Abstract
PDF(618K)
References
45
Martinot-Peignoux M, Stern C, Ripault M-P, et al. Twelve weeks post-treatment follow-up is as relevant as 24 weeks to determine the SVR in patients with HCV receiving PEG-IFN and ribavirin. Hepatology 2010; 51: 1122–6.
ChemPort
46
Sarrazin C, Berg T, Ross RS, et al. Prophylaxis, diagnosis and therapy of hepatitis c virus (HCV) infection: the German guidelines on the management of HCV infection. Z Gastroenterol 2010; 48: 289–351.
ChemPort
47
Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alpha-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002; 347: 975–82.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 2548
48
Davis GL, Wong JB, McHutchison JG, et al. Early virologic response to treatment with peginterferon alpha-2b plus ribavirin in patients with chronic hepatitis C. Hepatology 2003; 38: 645–52.
Direct Link:
Abstract
PDF(129K)
References
49
Ferenci P, Fried MW, Shiffman ML, et al. Predicting sustained virological responses in chronic hepatitis C patients treated with peginterferon alpha-2a (40 KD)/ribavirin. J Hepatol 2005; 43: 425–33.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 200
50
Berg T, von Wagner M, Nasser S, et al. Extended treatment duration for hepatitis C virus type 1: comparing 48 versus 72 weeks of peginterferon-alpha-2a plus ribavirin. Gastroenterology 2006; 130: 1086–97.
PubMed,
ChemPort,
Web of Science® Times Cited: 202
51
Berg T, Sarrazin C, Herrmann E, et al. Prediction of treatment outcome in patients with chronic hepatitis C: significance of baseline parameters and viral dynamics during therapy. Hepatology 2003; 37: 600–9.
PubMed,
ChemPort,
Web of Science® Times Cited: 119
52
Sánchez-Tapias JM, Diago M, TeraViC-4 Study Group et al. Peginterferon-alfa2a plus ribavirin for 48 versus 72 weeks in patients with detectable hepatitis C virus RNA at week 4 of treatment. Gastroenterology 2006; 131: 451–60.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 153
53
Sarrazin C, Schwendy S, Möller B, et al. COMPLETELY Individualized treatment durations (24, 30, 36, 42, 48, 60 OR 72 Weeks) with peginterferon-alfa-2B and ribavirin in hcv genotype 1-infected patients (INDIV-2 STUDY). J Hepatol 2010; 52 (Suppl. 1): S25–6.
CrossRef,
Web of Science®
54
Afdhal N, Levine R, Brown R, et al. Colchicine versus PEG-Interferon alpha 2b long term therapy: results of the 4 year copilot trial. J Hepatol 2008; 48(Suppl. 2): S4.
55
Di Bisceglie AM, Shiffman ML, Everson GT, et al. HALT-C Trial Investigators. Prolonged therapy of advanced chronic hepatitis C with low dose peginterferon. N Engl J Med 2008; 359: 2429–41.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 88
56
Bruix J, Poynard T, Colombo M, et al. Pegintron maintenance therapy in cirrhotic (Metavir F4) HCV patients, who failed to respond to interferon/ribavirin (IR) therapy: final results of the EPIC3 cirrhosis maintenance trial. J Hepatol 2009; 50: A49.
57
Zeuzem S, Buti M, Ferenci P, et al. Efficacy of 24 weeks treatment with peginterferon alpha-2b plus ribavirin in patients with chronic hepatitis C infected with genotype 1 and low pretreatment viremia. J Hepatol 2006; 44: 97–103.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 184
58
Jensen DM, Morgan TR, Marcellin P, et al. Early identification of HCV genotype 1 patients responding to 24 weeks peginterferon alpha-2a (40 kd)/ribavirin therapy. Hepatology 2006; 43: 954–60.
Direct Link:
Abstract
Full Article (HTML)
PDF(416K)
References
59
Ferenci P, Laferl H, Scherzer TM, et al. Peginterferon alpha-2a and ribavirin for 24 weeks in hepatitis C type 1 and 4 patients with rapid virological response. Gastroenterology 2008; 135: 451–8.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 53
60
Hadziyannis SJ, Sette Jr H, Morgan TR, et al. Peginterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C: a randomized study of treatment duration and ribavirin dose. Ann Intern Med 2004; 140: 346–55.
PubMed,
ChemPort,
Web of Science® Times Cited: 1076
61
Nasta P, Gatti F, Puoti M, et al. Insulin resistance impairs rapid virologic response in HIV/hepatitis C virus coinfected patients on peginterferon-alpha-2a. AIDS 2008; 22: 857–61.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 16
62
Kau A, Vermehren J, Sarrazin C. Treatment predictors of a sustained virologic response in hepatitis B and C. J Hepatol 2008; 49: 634–51.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 41
63
Pearlman BL, Ehleben C, Saifee S. Treatment extension to 72 weeks of peginterferon and ribavirin in hepatitis c genotype 1-infected slow responders. Hepatology 2007; 46: 1688–94.
Direct Link:
Abstract
Full Article (HTML)
PDF(216K)
References
64
Mangia A, Minerva N, Bacca D, et al. Individualized treatment duration for hepatitis C genotype 1 patients: A randomized controlled trial. Hepatology 2008; 47: 43–50.
PubMed,
ChemPort,
Web of Science® Times Cited: 82
65
Ferenci P, Laferl H, Scherzer TM, et al. Customizing treatment with peginterferon alpha-2a (40KD) plus ribavirin in patients with HCV genotype 1 or 4 infection: interimresults of a prospective randomized trial. Hepatology 2006; 44: 336A.
66
Buti M, Lurie Y, SUCCESS Study Investigators et al. Randomized trial of peginterferon alfa-2b and ribavirin for 48 or 72 weeks in patients with hepatitis C virus genotype 1 and slow virologic response. Hepatology 2010; 52: 1201–7.
Direct Link:
Abstract
Full Article (HTML)
PDF(197K)
References
67
Shiffman ML, Suter F, Bacon BR, et al. Peginterferon alpha-2a and ribavirin for 16 or 24 weeks in HCV genotype 2 or 3. N Engl J Med 2007; 357: 124–3.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 164
68
Dalgard O, Bjoro K, Hellum KB, et al. Treatment with pegylated interferon and ribavarin in HCV infection with genotype 2 or 3 for 14weeks: a pilot study. Hepatology 2004; 40: 1260–5.
PubMed,
ChemPort,
Web of Science® Times Cited: 155
69
von Wagner M, Huber M, Berg T, et al. Peginterferon-alpha-2a (40KD) and ribavirin for 16 or 24 weeks in patients with genotype 2 or 3 chronic hepatitis C. Gastroenterology 2005; 129: 522–7.
PubMed,
ChemPort,
Web of Science® Times Cited: 201
70
Mangia A, Santoro R, Minerva N, et al. Peginterferon alpha-2b and ribavirin for 12 vs. 24 weeks in HCV genotype 2 or 3. N Engl J Med 2005; 352: 2609–17.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 294
71
Yu ML, Dai CY, Huang JF, et al. A randomised study of peginterferon and ribavirin for 16 versus 24 weeks in patients with genotype 2 chronic hepatitis C. Gut 2007; 56: 553–9.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 88
72
Dalgard O, Bjoro K, Ring-Larsen H, et al. Pegylated interferon alpha and ribavirin for 14 versus 24 weeks in patients with hepatitis C virus genotype 2 or 3 and rapid virological response. Hepatology 2008; 47: 35–42.
Direct Link:
Abstract
Full Article (HTML)
PDF(211K)
References
73
Diago M, Shiffman ML, Bronowicki JP, et al. Identifying hepatitis C virus genotype 2/3 patients who can receive a 16-week abbreviated course of peginterferon alfa-2a (40KD) plus ribavirin. Hepatology 2010; 51: 1897–903.
Direct Link:
Abstract
Full Article (HTML)
PDF(168K)
74
Andriulli A, Dalgard O, Bjoro K, et al. Short-term treatment duration for HCV-2 and HCV-3 infected patients. Dig Liver Dis 2006; 38: 741–8.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 15
75
Mangia A, Ricci GL, Persico M, et al. A randomized controlled trial of pegylated interferon alpha-2a (40 KD) or interferon alpha-2a plus ribavirin and amantadine v. interferon alpha-2a and ribavirin in treatment-naive patients with chronic hepatitis C. J Viral Hepat 2005; 12: 292–9.
Direct Link:
Abstract
Full Article (HTML)
PDF(134K)
References
76
Willems B, Hadziyannis SJ, Morgan TR, et al. Should treatment with peginterferon plus ribavirin be intesified in patients with genotype 2/3 without a rapid virological response? # 8. J Hepatol 2007; 46(Suppl. 1): S6.
77
Sarrazin C, Shiffman ML, Hadziyannis SJ, et al. Definition of rapid virologic response with a highly sensitive real-time PCR-based HCV RNA assay in peginterferon alfa-2a plus ribavirin response-guided therapy. J Hepatol 2010; 52: 832–8.
CrossRef,
ChemPort,
Web of Science® Times Cited: 1
78
Neumann AU, Pianko S, Zeuzem S, et al. Positive and negative prediction of sustained virologic response at weeks 2 and 4 of treatment with albinterferon alfa-2b or peginterferon alfa-2a in treatment-naïve patients with genotype 1, chronic hepatitis C. J Hepatol 2009; 51: 21–8.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 5
79
Martinot-Peignoux M, Maylin S, Moucari R, et al. Virological response at 4 weeks to predict outcome of hepatitis C treatment with pegylated interferon and ribavirin. Antivir Ther 2009; 14: 501–11.
PubMed,
ChemPort,
Web of Science® Times Cited: 7
80
Mihm U, Herrmann E, Sarrazin C, Zeuzem S. Review article: predicting response in hepatitis C virus therapy. Aliment Pharmacol Ther 2006; 23: 1043–54.
PubMed,
ChemPort,
Web of Science® Times Cited: 17
81
Ge D, Fellay J, Thompson AJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature 2009; 461: 399–401.
CrossRef,
ChemPort,
Web of Science® Times Cited: 160
82
Thompson AJ, Muir AJ, Sulkowski MS, et al. Interleukin-28B Polymorphism Improves Viral Kinetics and Is the Strongest Pretreatment Predictor of Sustained Virologic Response in Genotype 1 Hepatitis C Virus. Gastroenterology 2010; 139: 120–9.
CrossRef,
ChemPort,
Web of Science® Times Cited: 7
83
Suppiah V, Moldovan M, Ahlenstiel G, et al. IL28B is associated with response to chronic hepatitis C interferonalpha and ribavirin therapy. Nat Genet 2009; 41: 1100–4.
CrossRef,
ChemPort,
Web of Science® Times Cited: 85
84
Tanaka Y, Nishida N, Sugiyama M, et al. Genome-wide association of IL28B with response to pegylated interferonalpha and ribavirin therapy for chronic hepatitis C. Nat Genet 2009; 41: 1105–9.
CrossRef,
ChemPort,
Web of Science® Times Cited: 95
85
Asselah T. Genetic polymorphism and response to treatment in chronic hepatitis C: the future of personalized medicine. J Hepatol 2010; 52: 452–4.
ChemPort
86
Kotenko SV, Gallagher G, Baurin VV, et al. IFN-lambdas mediate antiviral protection through a distinct class II cytokine receptor complex. Nat Immunol 2003; 4: 69–77.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 325
87
Mangia A, Thompson AJ, Santoro R, et al. An IL28B polymorphism determines treatment response of hepatitis C virus genotype 2 or 3 patients who do not achieve a rapid
No comments:
Post a Comment