Posted: 12/18/2011; Future Virology. 2011;6(11):1361-1376. © 2011 Future Medicine Ltd.
Abstract
Many glomerular diseases can be caused by viral infections based on the diagnostic criteria, including clinical and laboratory data, and molecular analysis of tissue. Operative pathogenetic mechanisms include kidney tropism of the virus, immune complex formation, direct cytopathogenic effect, and multi-organ failure. Chronic infection with hepatitis virus is etiologically linked to well-defined glomerulopathies. In endemic areas, HBV is associated with both membranous nephropathy and mesangiocapillary glomerulonephritis, while HCV is known to cause cryoglobulinemia-mediated glomerulonephritis and other forms of glomerulonephritis. Renal biopsy with appropriate serological and molecular testing helps to define virus-related glomerular lesions and provides a prognostic and therapeutic guide. Antiviral agents remain the mainstay of treatment.
Introduction
It is not easy to establish the pathogenic links between an infection and renal disease, as there are complex criteria for proving such causality. Often, one has to recognize the clinical syndrome, to integrate the serological finding, identify specific antigens related to the infective organism and demonstrate the presence of an infective organism or its antigen(s) and host antibodies in glomerular/tubular structures. According to Koch's postulate, the etiological link should be confirmed by complete cure following eradication of the infective organism, an event that is, however, not always possible, especially in viral infection. In contrast to acute bacterial infection, chronic viral infection is characterized by higher concentrations of tissue viral antigens than in the circulation, where they are complexed with specific antibodies. Recently, identification of the virus in pathological tissue by techniques such as in situ hybridization, PCR and ultrastructural analysis has often been successful in demonstrating the presence of virus. A note of caution should be introduced, however, as the tubular uptake of viral particles is common, and this occurrence does not necessarily indicate the presence of an etiological link to renal disease. Clearance of the suspected antigen occurring simultaneously with clinical remission, or glomerulonephritis (GN) recurrence following reinfection can often provide support for such etiological association.
Many forms of infection may be complicated by GN or interstitial nephritis, although only a minority of patients will be involved. Some patients will develop chronic kidney disease, especially when persistent infection occurs. Infection remains an important etiology of chronic kidney disease in developing and underdeveloped countries. The most frequent and long-recognized virus-related glomerulopathies are those associated with HBV, while cryoglobulinemia-related mesangiocapillary glomerulonephritis (MCGN) has traditionally been related to HCV infection. This chapter focuses on HBV- and HCV-related glomerulopathies.
Historical Perspective
Following the landmark discovery in 1965 of the Australian antigen, subsequently renamed the hepatitis B surface antigen (HBsAg), Combes and coworkers first described the occurrence of membranous nephropathy (MN) due to glomerular deposition of Australian antigen-containing immune complexes in a 53-year-old man in 1971.[1] Different histological types of glomerular lesions have since been described in association with HBV infection; however, the most striking is still MN.
HBV Virology
HBV is a hepatotropic, double-stranded DNA virus of the Hepadnaviridae family. HBV has a double-shelled virion 42–47 nm in diameter, a 27-nm internal core, an excess of incomplete 22-nm spheres, and a circular DNA genome with a length varying between 3,000 and 3,300 base pairs. The DNA genome contains only 4 genes that encode viral proteins. These include the surface (S) gene, which encodes the 3 forms of HBsAg, the precore/core (PC/C) gene, which encodes the core protein and hepatitis B e antigen (HBeAg), the X gene, which encodes the X protein, and the polymerase (P) gene, which encodes the viral DNA polymerase. HBV is itself not cytopathic, but hepatitis often develops due to the host's immune reaction toward infected hepatocytes. HBV utilizes a replication strategy closely related to retroviruses, in that transcription of RNA into DNA is a critical step. Unlike the mechanisms observed in retroviral infection, HBV replication does not involve the integration of viral DNA into host cell DNA. Once an HBV particle has bound to and entered a hepatocyte, the HBV DNA enters the cell nucleus, where it is converted into covalently closed circular DNA, a highly stable structure that acts as an intermediate template for RNA copy transcription. This pregenomic mRNA is transported to the cytoplasm, where it carries out two functions: serving as a template for the synthesis of new HBV DNA and containing the genetic information necessary for directing viral protein synthesis.
Epidemiology
Today, HBV infects 350–400 million people worldwide. HBV-related nephropathy prevalence, particularly MN, follows geographic HBV prevalence patterns closely. HBV infection occurs throughout the world and is endemic in developing countries, such as Africa, eastern Europe, the Middle East, central Asia, China, southeast Asia, the Pacific Islands and the Amazon basin of South America (prevalence rates up to 10% or higher).
Vertical transmission from mother to child predominates in endemic areas. In nonendemic areas, horizontal transmission can occur via mucous membranes (e.g., sexual contact), via direct blood–blood contact (e.g., during blood transfusion) or via contact with blood or body fluids and the percutaneous route (e.g., needle-sharing practices in illicit intravenous drug use).
Definition of HBV-related GN
The pathogenetic role of HBV in renal disease has attracted much attention, since Combes et al. [1] in 1971 reported GN with immune complexes of HBsAg and its antibody (anti-HBs) in a patient infected with HBV. Previous observations of a greater-than-expected incidence of chronic HBsAg carriers among the patients with various forms of glomerulonephritides compared with the general hospital population in different geographic areas tend to support the hypothesis of a pathogenetic association between chronic HBV infection and GN.[2,3] Various morphological patterns including MN, MCGN, minimal change nephropathy and mesangial proliferative GN have since been described.[2,3]
The only definitive means to prove that a particular GN is etiologically associated with chronic HBV infection is to fulfill the following criteria:
- The pathology should be reproducible in experimental animals infected with the virus;
- Demonstration of HBV-specific antigen(s) and/or genome in the glomerulus;
- Disappearance of the pathological lesion with eradication of the virus.
Unfortunately, solid research work reproducing GN in infected experimental animals was lacking until recently. Inoculating primates with varying amounts of human plasma containing HBsAg resulted in lesions consisting of progressive focal GN with mesangial alterations that developed over a period of 4–10 months after inoculation. The most likely explanation is immune complex deposition. The possibility that the immune complex deposition may have resulted from an antibody response to human plasma that was injected can be excluded, since in rabbits injected with a single dose of bovine serum albumin any renal lesions were reversible and undetectable by the 4th week after injection. In the primates the renal lesions were progressive, and a temporal progression of these lesions was observed, which was similar to that reported in the chronic bovine serum albumin-rabbit model.
Observations from chronic woodchuck hepatitis virus infection in woodchucks revealed three types of GN, namely: MN with capillary hepatitis B core antigen (HBcAg) deposits, mesangial proliferative glomerulonephritis with mesangial deposits of HBsAg, and mixed membranous and mesangial proliferative GN with capillary deposits of HBcAg and mesangial deposits of HBsAg.[4] The animal model of woodchuck hepatitis may be valuable for experimental study of the natural progression of renal lesion, as their pathological findings are similar to those of humans. Membranous nephropathy is the most common type of GN in humans and is particularly frequent in male children.[3] Mesangial proliferative forms with IgA deposits appear to be more common in adults.[2] Woodchucks with a membranous component appeared to be younger, whereas woodchucks with mesangial proliferative GN appeared to be older. Affected animals were predominantly male as compared with that of the chronic carrier population. Thus, the pattern of occurrence of these types of GN was similar to that observed in human kidneys, with the exception of HBeAg, as the woodchuck hepatitis antigen system has not been characterized.
Complete disappearance of the pathology with eradication of the virus in human beings is not easily demonstrated because of the ethical consideration of renal biopsy in patients in clinical remission. Hence, the diagnosis of HBV-related GN, at present, depends on the demonstration of HBV specific antigen(s) in the glomeruli.
Pathology of HBV-related GN
Membranous nephropathy remains the best-recognized glomerulopathy associated with chronic HBV infection. Coexistence of mesangial proliferative GN with mesangial IgA deposits was first reported in five chronic HBsAg carriers by Nagy et al. [5] and later in two patients by Sluzarczk et al..[6] Mesangial IgA nephropathy associated with chronic HBV infection was subsequently supported by other investigators.[7] MCGN is also a well recognized glomerulopathy associated with chronic HBV infection.
The association between chronic HBV infection and other renal pathologies such as focal glomerulosclerosis, minimal change nephropathy and polyarteritis nodosa (PAN) remains unclear. Focal glomerulosclerosis in HBsAg carriers is likely to be secondary to progression of other types of HBV-related GN or a sequel of hepatic cirrhosis. Although minimal change nephropathy has been reported in chronic HBV carriers, the pathogenetic association is unlikely, as glomerular deposition of immunoglobulin and HBV antigen is rarely observed. Furthermore, the prevalence of hepatitis B surface antigenemia in nephrotic patients with minimal change nephropathy is not higher than that of the general population.[2] The intriguing association between PAN and hepatitis B was first reported in 1970. Subsequently, the incidence of HBsAg carriers amongst various series has been noted in 0–54% of cases of PAN (reviewed by Johnson and Couser[3]). Of interest is the observation that PAN associated with hepatitis B has been primarily reported in Europe and the USA, where infection is usually acquired via a parenteral route and with higher prevalence of HBsAg carrier state in adults. In contrast, PAN associated with hepatitis B is uncommon in endemic areas such as southeast Asia and Africa, where most infection occurs in childhood via transmission from parents or siblings. Furthermore, the variability in incidence of HBsAg in PAN within the USA may be accounted by the different prevalence of intravenous drug abuse and the HBV carrier rate at the various reporting centers. For example, up to 40% of PAN is HBV associated in New York, USA, as opposed to Ann Arbor, MI, USA, and Rochester, MN, USA, where the rates range from 6 to 25%.[3] A review of PAN and microscopic polyangiitis failed to demonstrate any association between HBV and systemic vasculitides.[8] Retrospective analysis of 115 patients with HBV-associated PAN revealed that when renal involvement is present, the pathology is vasculitic with no cases of glomerulonephritides.[9] Despite these observations, the etiological association between chronic HBV infection and PAN/microscopic polyangiitis has not been substantiated.
Nature of HBV Antigens in Glomeruli
HBV-associated GN is an immune complex-mediated disease. Three distinct antigens, HBsAg, HBcAg, and HBeAg have been detected by immunofluorescence studies in renal biopsies from patients with HBV-associated GN. Both HBcAg and HBsAg have a molecular weight in excess of 2 million Da. HBeAg, which is a part of the viral nucleoprotein derived from denatured HBcAg, is found in two forms with molecular weights of 19,000 and 300,000 Da. HBeAg is capable of inducing MN by being preferentially deposited along capillary walls.[10] If HBV antigens with a lower molecular weight (i.e., HBeAg) induce MN, one would predict that mesangial proliferative or MCGN associated with chronic HBV infection would show immune complexes with high molecular weight antigens (i.e., HBsAg). Furthermore, a mixed picture of mesangial IgA and MN should be seen in HBV-related GN, since immune complexes with different molecular weights may be present simultaneously in some of these patients. Such a glomerulopathic entity has been reported with mesangial HBsAg and capillary HBeAg deposits,[11,12] thus confirming the aforementioned hypothesis and also agreeing with the experimental findings of Germouth et al..[13]
HBV-related MN
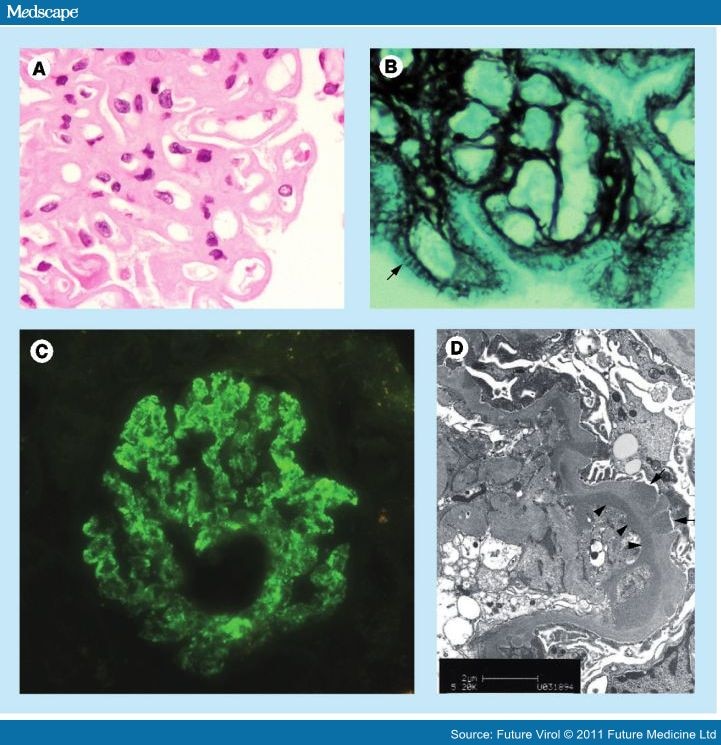
Glomerular capillary depositions of HBsAg, HBcAg, and HBeAg in HBV-related MN nephropathy have been observed by various investigators using different reagents. Hirose et al. had used F(ab')2 fragments of anti-HBsAg monoclonal antibody to demonstrate that capillary deposits were HBeAg in nature.[12] Using the same F(ab')2 fragment of anti-HBeAg monoclonal antibody and another monoclonal antibody against HBeAg, Lai et al. demonstrated capillary HBeAg deposits in two-thirds of the biopsies,[14] and the incidence was similar to that reported by Hirose et al..[12] However, identical capillary HBeAg immunostaining was demonstrated when polyclonal antibody was used.[14] Further studies revealed that commercial polyclonal anti-HBeAg antiserum contains both anti-HBeAg and anti-HBcAg activity (Figure 1C).[14] This can be explained by the fact that the HBeAg is an integral component of HBcAg.
 Figure 1.
Figure 1.HBV-related Mesangial Proliferative GN With Mesangial IgA Deposits Lai et al. reported the detection of glomerular HBsAg by polyclonal antisera in 30% of renal biopsies from HBsAg carriers with IgA nephropathy.[2] Contrary to the pathologic findings in HBV-related MN, glomerular HBeAg deposits were not detected in the renal biopsies taken from these chronic HBsAg carriers with IgA nephropathy using both polyclonal and monoclonal antibodies. Instead, mesangial deposits of HBsAg similar to the distribution of IgA immunostaining were detected in 40% and 21% of the renal biopsies by polyclonal and monoclonal antibodies, respectively,[14] suggesting that HBsAg rather than HBeAg may play a pathogenetic role in some of the patients with IgA nephropathy associated with chronic HBV infection.
HBV-related MCGN Well documented reports of such glomerulopathic entities both demonstrated simultaneous glomerular deposition of HBeAg and HBsAg,[15] supporting the hypothesis that immune complexes with HBV antigens of different molecular weights could induce a mixed pattern of GN as shown previously in cases of mixed IgA and MN.[11]
Immunopathology of HBV-related GN
Animal experiments and observations on human subjects have demonstrated that HBV-containing immune complexes may be formed in the course of HBV-induced acute and chronic hepatitis. Immune complex-mediated GN requires a continuous supply of antigen and a sustained antibody response, and, apparently, these requirements seem to be met in chronic HBV carriers. Despite the detection of circulating immune complexes in HBV-related MN, circulating immune complexes containing HBV antigen(s) as an integral part have not been unequivocally demonstrated in these patients. This raises the possibility of immune complex formation in situ (which occurs in primary MN) in HBV-related MN.
Extrahepatic HBV replication occurs in human subjects, but it is unclear whether viral replication occurs within the kidney in those patients with HBV-related GN. Virus-like particles of 40–50 nm diameter have been demonstrated within the glomerular electron-dense deposits in renal biopsies from patients with HBV-related GN. HBV viral replication in the kidneys of some of these HBV-related GN is suggested by the localization of HBV DNA genome by in situ hybridization in glomeruli.[16,17] This mechanism is supported by findings in woodchucks. De novo synthesis of viral antigens in viral infection has been demonstrated in renal tissues of woodchucks, and small amounts of viral-specific mRNA, including full-length transcripts, have been demonstrated in the glomeruli of woodchuck hepatitis virus-infected woodchucks.[18]
Lin had detected HBV DNA in glomeruli and tubular epithelia by in situ hybridization in patients with early-onset HBV-related MN, but the glomerular HBV DNA was exclusively extracellular.[19] It is plausible that such presence of HBcAg or HBV DNA results from endocytosis by proximal tubular epithelia when the HBV DNA in the urinary filtrate crosses their luminal borders. Alternatively, the presence of HBV DNA in the tubular epithelia could indicate HBV replication in the tubular epithelia, and these findings are in keeping with other transgenic mouse studies revealing the expression of viral genome of HBcAg or HBeAg only in tubular epithelial cells.[20] Using PCR and in situ hybridization, Lai et al. demonstrated that HBV DNA was frequently present in the cytoplasm of renal proximal tubules in different HBV-related glomerulonephritides of long duration.[21] More importantly, they detected transcriptionally active HBV genomes or mRNA in the glomeruli in biopsies from HBV-related glomerulonephritides by in situ hybridization with a HBV-specific RNA probe. The HBcAg mRNA was localized mainly in epithelial cells in HBV-related MN, and in both epithelial and mesangial cells in HBV-related IgA nephropathy. These findings strongly suggest the notion that nephropathy may arise from immune complex formation in situ.
Clinical Findings
Symptoms & Signs
Pediatric and adult patients tend to have slightly different clinical manifestations of HBV-related MN (Table 1). There is a strong male preponderance in children in pediatric HBV-related MN and nephrotic syndrome is the most frequent presentation. A small proportion presents with microscopic hematuria with normal or mildly impaired renal function. Pediatric carriers of chronic HBV often do not have overt liver disease, and transaminase levels are usually normal. In adult patients, the most common manifestations are the nephrotic syndrome or proteinuria. The preponderance of occurrence in adult males is less obvious compared to that which is observed in children. In addition, adults are more likely to suffer from hypertension, renal dysfunction and clinical evidence of liver disease than children.
HBV-related MN has a favorable prognosis in children, with several high-prevalence areas reporting stable renal function and high rates of spontaneous remission, including Hong Kong, South Africa and Turkey.[22] On the other hand, adults with HBV-related MN usually develop progressive disease. In Hong Kong, for example, up to 29% of patients experienced progressive renal failure, while a further 10% developed end-stage renal disease over 5 years.[23] In patients with nephrotic-range proteinuria and overt hepatitis at presentation, the prognosis is even worse, with over 50% of patients requiring renal replacement therapy over 3 years.[24] Prognosis is worse in those with vertical versus those with horizontal transmission and is also worse in endemic versus sporadic infection.
Laboratory & Pathologic Findings
Laboratory tests including standard liver biochemistries (serum alanine aminotransferase, γ-glutamyltransferase and bilirubin levels), and HBV serologies (HBsAg, HBeAg, anti-HBe and anti-HBc antibodies) should be monitored for diagnostic purposes and also to assess response to treatment. HBeAg is present in 80% of patients, who may also have high titers of anti-HBc. When biochemical hepatitis is observed, subjects should also be tested for circulating HBV DNA levels, and undergo liver biopsy. In addition, an α-fetoprotein assay could be a useful supplementary diagnostic. Serum C3 and C4 levels may be low in 20–50% of patients.
Light microscopic findings are similar to those of idiopathic MN, with some differentiating features (Figure 1). The characteristic glomerular lesion is a diffuse thickening of glomerular capillary walls to form thick 'membranes' (Figure 1A). It is now firmly established that this alteration is caused by immune complexes that accumulate subepithelially on the outer aspect of the glomerular basement membrane (GBM) that assumes the 'membranous' morphology in a stepwise manner. Other pertinent light microscopic findings are reflected by the reactive structural changes of the GBM induced by immune complexes. Therefore, special stains highlighting the GBM, like methenamine silver and periodic acid-Schiff (PASM or silver stain) or trichrome stain, are more useful. The earliest change on silver staining is a mottled appearance best seen on tangential sections and represents slight indentations of the GBM by immune complexes adhering to its surface. The most specific change of the GBM is the so-called 'spike' formation (Figure 1B). These are projections of GBM material between immune complexes that lead to a sawtooth-like appearance of the GBM. This pattern is pathognomonic of full-blown MN. Disease progression results in a diffuse thickening of the GBM. The major constituents of the immune complexes are IgG together with C3; IgM, IgA and C1q may be present. Ultrastructural findings typically consist of both subepithelial and occasional subendothelial deposits (Figure 1D). The presence of subendothelial deposits, sometimes referred to as MCGN type III changes, increases the likelihood that a case of MN is secondary (e.g., HBV-related) rather than idiopathic. The presence of mesangial proliferation on light microscopy is helpful in distinguishing this form of secondary MN from idiopathic MN.
The light microscopic finding of HBV-related mesangial proliferative GN with mesangial IgA deposits resembles that of primary IgA nephropathy. Regardless of the pathologic finding, it is important to locate HBV-specific antigens in the biopsy. To document an etiologic association between HBV and MN or other forms of glomerular lesion, demonstration of HBV-specific antigens by immunofluorescence is indispensable. Furthermore, HBV DNA and mRNA have been detected in the glomerulus and tubular epithelia by PCR and in situ hybridization with specific HBV RNA probes.[21]
Treatment
Unlike childhood disease, in which there is a high rate of spontaneous remission,[25] adults with HBV-related MN typically undergo a progressive course of the disease.[23] As yet, an ideal therapeutic agent has not been discovered. Ideally, treatment for HBV-related glomerular disease should accomplish the following objectives:
- Amelioration of nephrotic syndrome and associated complications, such as hyperlipidemia, edema, infection and venous thrombosis;
- Renal function preservation;
- Liver function normalization and the prevention of HBV-related hepatic complications;
- Permanent eradication of HBV.
Given the disease's immune complex nature, it was once fashionable to make use of immunosuppressive therapy, similar to that used in the idiopathic form of the disease. Although corticosteroids had been previously reported to provide symptomatic relief in isolated cases, the current view is that such steroids and cytotoxic agents may harm more than they help, by causing deleterious hepatic flares or even fatal decompensation due to enhanced viral replication upon treatment withdrawal.[26]
Antiviral agents have emerged as an important therapeutic option. IFN-α is a naturally occurring cytokine produced by B-lymphocytes, null lymphocytes and macrophages, and possesses antiviral, antiproliferative and immunomodulatory effects. While reported to be useful in children, IFN-α has produced mixed results in adults with HBV-related MN.
The treatment of chronic HBV infection has been revolutionized by the introduction of the nucleoside analog lamivudine. Unfortunately, however, prolonged treatment with lamivudine may be limited by the potential emergence of drug-resistant strains due to the induction and selection of HBV variants with mutations at the YMDD motif of their DNA polymerase. An alternative agent that could be considered for use in such lamivudine-resistant cases is adefovir dipivoxil, an acyclic nucleotide analog. This agent is effective against both lamivudine-resistant and wild-type HBV. This agent is potentially nephrotoxic, however, and as yet there has been no clinical trial regarding its efficacy in the treatment of HBV-related MN nonresponsive to lamivudine treatment. There is data to suggest that the recommended dose of 10 mg adefovir dipivoxil is associated with a lower risk of nephrotoxicity.[27]
Unlike chronic liver disease due to hepatitis B, for which well-designed placebo-controlled clinical trials (CCTs) are available, studies on the treatment of HBV-related GN are usually case reports or small-sample uncontrolled trials. In order to draw a reliable conclusion, such clinical trials should fulfill a set of criteria including the results of primary antiviral therapy, the virological response (VR) and clinical response as a clinical end point. The overall estimate for sustained remission of proteinuria induced by interferon therapy in five CCTs, case–control or cohort studies was 50%.[23,28–31] Chronic HBV carriers with normal renal function typically have better response. In the general population, interferon therapy clears HBeAg from serum in 30–40% of patients with chronic hepatitis B infection.[32] It appears that the response rate is higher in children and adult patients from nonendemic areas. The natural history of HBV-related nephrotic syndrome in children tends to show gradual improvement in many cases. For patients from nonendemic areas, the shorter duration of infection may favor a better VR to antiviral therapy. However, patients from endemic areas who acquire HBV infection as neonates or at very young age and those with chronic renal insufficiency at diagnosis tend to have less favorable response to interferon therapy.
Table 2 summarizes nine reports (one CCT and eight case reports) on the therapeutic effect of lamivudine in HBV-related GN.[33–41] The overall clinical and VRs with lamivudine were better than that of interferon. The link between sustained proteinuria remission and HBeAg clearance was stronger with lamivudine-based studies than interferon-based studies.
The efficacy and safety of adefovir dipivoxil were examined in six patients with HBV-associated GN.[42] After 1 year of treatment (100 mg daily), the disease subsided fully in three patients (50%) and partially in two. The negative conversion rates of HBV DNA and HBeAg at 6 months were 83.3% and 66.7% respectively. These findings suggest a therapeutic value of adefovir dipivoxil in HBV-associated GN, but an optimal dosage must first be established to prevent nephrotoxicity.[27]
Prevention
Previously, lacking an ideal agent for the treatment of HBV-related glomerulopathy, active immunization remained the most effective measure of immunoprophylaxis. Prevention by an effective vaccination program is still far superior to antiviral treatment despite the promising new antiviral therapies. These medications are expensive and the treatment period is prolonged, with no consensus opinion of treatment duration. Vaccination for all newborns in some endemic areas has dramatically reduced the incidence of chronic HBV infection and its associated complications in children and adolescents. In Taiwan, active immunization of all newborns since 1984 has led to a dramatic (tenfold) decline in the incidence of neonatal HBV infection and its subsequent sequelae.[43] A study from Shanghai in China revealed that only 3.5% of vaccinated children developed HBV-related GN as compared with 12.6% of nonvaccinated children.[44] Furthermore, the incidence of HBV-related GN fell by 50% within 10 years of the introduction of a vaccination program in an endemic region. A similar fall in the incidence rate of HBV-related MN was reported in the pediatric population in South Africa.[45] In 2003, WHO recommended that all countries provide universal HBV immunization programs for infants and adolescents.[46]HCV-related GNHistorical Perspective
In 1966, Meltzer and coworkers first described the clinical manifestations associated with 'mixed' cryoglobulinemia.[47] They described a clinical triad that consisted of palpable purpura, arthralgias and weakness plus variable degrees of GN, lymphadenopathy, and hepatosplenomegaly in some patients. Cryoglobulinemia in these patients had a 'mixed' composition of IgG and IgM rheumatoid factor (RF). The cause of this disease was entirely a mystery in those days, and its association with HCV infection only became increasingly apparent following its discovery in 1989.[48,49] It is now apparent that the classical clinical triad only occurs in a minority of patients. The most common manifestation is the markedly heterogeneous presentations of systemic vasculitis, with purpuric skin lesions that show leukocytoclastic vasculitis on biopsy being an almost constant and predominant feature of HCV virology.
HCV is a small RNA virus of the Flaviviridae family and has been recently classified as the sole member of the genus hepacivirus.[50] The virus is a small double-shelled virus consisting of a lipid envelope (E) with virally encoded glycoproteins (E1 and E2) and an inner nucleocapsid (core) that contains a positive-sense single-stranded RNA genome of 9,500 nucleotides. It has well-defined structural (core, E1 and E2) as well as several nonstructural (NS2–NS5) proteins. The nonstructural proteins encode several proteases, a virus-specific helicase and an RNA-dependent RNA polymerase responsible for replication of the genome. Six major genotypes based on sequence homology, and more than 50 subtypes, have emerged from the evolution of HCV.[51]
Epidemiology
To date, WHO has estimated approximately 170–200 million individuals worldwide have chronic HCV infection.[52] HCV infection is not confined to the liver and a wide variety of extrahepatic disease manifestations have been reported. The exact prevalence of extrahepatic diseases is not known but HCV is definitely involved in nonhepatic pathological processes.
There are two immunologic features of HCV that may predispose patients to experiencing manifestations of extrahepatic disease. First, it is known that HCV evades immune elimination, leading to chronic infection and the accumulation of circulating immune complexes exemplified by MCGN associated with HCV infection. The second feature is that HCV stimulates production of monoclonal rheumatoid factors (mRF). This feature causes type II cryoglobulinemia that is responsible for most of the symptomatic cryoglobulinemic vasculitis. Despite its lower occurrence, one should note that extrahepatic involvement of chronic HCV infection is responsible for much of the increased morbidity and mortality accompanying the disease.
The prevalence of mixed cryoglobulinemia increases with the duration of the hepatitis infection. Chronic hepatitis C carriers with mixed cryoglobulinemia have an apparent duration of disease that is almost twice as long as those without cryoglobulinemia.[53] A high prevalence of mixed cryoglobulinemia (35–90%) has been reported for patients with HCV infection.[54,55] However, in assessing the prevalence of mixed cryoglobulinemia, it is important to realize that prevalence has not been determined in populations of unselected HCV-infected patients. Hence, reports of high prevalence of mixed cryoglobulinemia may represent a selection bias (e.g., studies on cirrhotic patients with long-standing HCV infection from gastroenterology centers). Overt symptomatic cryoglobulinemia occurs in 1% or less of patients, and is usually associated with high RF and cryoglobulin titers. The testing of unselected patients with cryoglobulinemia has revealed an anti-HCV antibody-positivity rate of up to 90%. While type I MCGN has been regarded as idiopathic for some time, chronic HCV infection is observed in a considerable proportion of patients. The exact proportion of patients with type I MCGN who are positive for anti-HCV antibody is unknown.
The most frequent form of renal involvement in HCV infection is MCGN, according to data from the USA and Japan.[56,57] The real prevalence of MCGN without detectable cryoglobulinemia is difficult to assess. Such cases might represent a subclinical form of cryoglobulinemia owing to a failure to detect circulating cryoglobulins due to technical issues in laboratory.[58] Furthermore, IgM antibodies with anti-IgG activity may induce immune complexes without cryoprecipitable properties.[58] Lastly, these patients may only develop detectable circulating cryoglobulinemia late in the course of the disease.[59]Definition of Cryoglobinemia
Cryoglobulinemia is defined as the presence in serum of immunoglobulins that precipitate at reduced temperatures. Therefore, blood samples obtained from patients for detection of cryoglobulins must be stored and transported at 37°C.
Brouet et al. classified three types of cryoglobulins based on their immunoglobulin (Ig) composition.[60] Type I consists of a single monoclonal Ig without antibody activity, and can be found in patients with multiple myeloma, Waldenström's macroglobulinemia, or idiopathic monoclonal gammopathy. Types II and III, or mixed cryoglobulins, consist of polyclonal IgG and monoclonal IgMκ (type II) or polyclonal IgM (type III) with RF activity (Table 3). When no definite disease association is found, the condition is referred to as essential mixed cryoglobulinemia. The observation that up to 90% of unselected patients with cryoglobulinemia have anti-HCV antibody indicates that the disease is not genuinely 'essential', but more likely related to HCV infection. Hence, the term 'essential' may be a misnomer and can no longer be used for the majority of cases, where cryoglobulins consist of complexes of RF, IgG, anti-HCV antibody and HCV virions.[61] The pathogenesis of cryoglobulinemia due to HCV infection is not well understood, but it appears to be related to excessive proliferation of B cells as a result of the chronic antigenic stimulation of HCV infection.[62]
Clinical Findings
Symptoms & Signs
HCV-related Cryoglobulinemia Full-blown symptomatic cryoglobulinemia occurs infrequently, and the typical symptoms are fatigue and palpable purpura, which histologically consists of leukocytoclastic vasculitis (with complexes of anti-HCV antibody and HCV in injured tissue). These lesions are usually found on the lower limbs, although they can occur anywhere, and represent small vessel vasculitis. A smaller proportion of patients have fever, arthritis, Raynaud's phenomenon and neuropathy. Peripheral neuropathy is usually characterized by paresthesias and variable degrees of motor deficit. Abdominal pain arises from mesenteric vasculitis, and may mimic an acute abdominal emergency during disease flare. Hepatosplenomegaly is due to chronic liver disease as a result of HCV. Cryoglobulinemia is more common in women than men and typically occurs after a prolonged period, often years or decades, of HCV infection. Although the course of illness tends to wax and wane, occasionally the systemic illness can be severe or even fulminant. For instance, nodular pulmonary infiltrates from deposition of cryoglobulins leading to respiratory failure, and non-Hodgkin's B-cell and splenic lymphomas have been reported to arise in the setting of cryoglobulinemia.[63] In addition, cryoglobulinemia has also been anecdotally reported in association with adenocarcinoma of the liver and stomach in Chinese individuals.[64]
Cryoglobulinemic GN The typical renal manifestation of HCV infection is MCGN type I, usually in the context of cryoglobulinemia.[56] Type II MCGN (e.g., dense deposit disease) has not been reported in association with HCV infection. MCGN associated with type II cryoglobulinemia is the predominant type of GN clinically associated with HCV infection in studies from Italy,[65] USA[66] and Japan.[57] The prevalence of MCGN in HCV-type II cryoglobulinemia is approximately 30%, yet the prevalence of anti-HCV antibody among patients with MCGN is much lower in Chinese populations.[67] MCGN also is occasionally observed in patients with hepatitis C in the absence of cryoglobulinemia.[56]
Renal disease is rare in children; the typical age of disease onset is 40–60 years old, following long-standing infection, and is often associated with mild subclinical liver disease. Patients may have other cryoglobulinemia symptoms, such as palpable purpura and arthralgias. Renal manifestations include nephrotic (20%) or non-nephrotic proteinuria and microscopic hematuria.[68] Acute nephritic syndrome is the presenting feature in 25% of cases. Progression to uremia is associated with male gender and old age. 50% of patients develop renal insufficiency, although this is frequently mild. Over 80% of patients have refractory hypertension at presentation, which may be a cause for the high rate of cardiovascular deaths.
The natural history of HCV-related cryoglobulinemia remains poorly defined. The clinical course can vary dramatically. The renal disease tends to have an indolent course without significant renal deterioration despite the persistence of urine abnormalities in the majority of patients. Around 15% of patients eventually require dialysis according to an Italian study.[69]
Laboratory Findings
The diagnosis of HCV-related MCGN is established by laboratory testing coupled with renal biopsy. Most patients are seropositive for anti-HCV antibody and HCV RNA. 70% have raised serum transaminase levels. Cryoglobulins are detected in 50–70% of patients. Serum electrophoresis and immunofixation reveals type II mixed cryoblobulins, in which the mRF, almost invariably an IgMκ, is a distinguishing feature of cryoglobulinemic GN. Their amount, usually measured as a cryocrit, varies from one patient to another, and varies from time to time in a given patient (ranging between 2% and 70%). It is common for urine κ light chains to be present. Clinical activity has little effect on the serum complement pattern, which is also discriminative. Low or even undetectable levels of the early complement components (C4 and C1q) and CH50 is characteristic, while the C3 level tends to remain normal or only slightly reduced.
Pathologic Findings
Renal histological evaluation typically shows evidence of immune complex deposition in glomeruli and changes in MCGN.[56] MCGN refers to a pattern of glomerular injury characterized by diffuse mesangial proliferation and thickening of the capillary wall, hence the synonym of membranoproliferative GN. In cryoglobulinemic MCGN, light microscopy reveals an increased number of mesangial cells, expansion of the mesangial matrix, and diffuse accentuation of glomerular tufts, which gives a lobular appearance to the glomeruli (Figure 2A). Glomerular capillary walls appear thickened because of the interposition of mesangial matrix between the GBM and the endothelium. Staining of the GBM with periodic acid-Schiff or silver stain shows splitting ('double contour') or 'tram-tracking' due to insertion of the mesangial matrix (Figure 2B). Immunofluorescence reveals granular deposits of C3 and IgG in the mesangium and in peripheral capillary loops (Figure 2C). A similar morphological appearance may be seen with infective endocarditis and infected ventriculoatrial shunts (shunt nephritis). In addition, glomerular capillaries may have marked inflammatory cell infiltrates with mononuclear cells and polymorphonuclear leukocytes, a distinguishing feature from noncryoglobulinemic MCGN. Intracapillary globular accumulations of eosinophilic material representing precipitated immune complexes or cryoglobulins may also be present. Viral HCV-containing antigens had been previously detected in glomerular structures using a three-stage indirect immunohistochemical monoclonal antibody technique,[70] but this was not confirmed by subsequent studies. Electron microscopy shows subendothelial deposits that may have a tactoid pattern, size, and distribution suggestive of cryoglobulin deposition. These tend to be of 15–30 µm in size, distinguishing them from the smaller fibrillary deposits (12–25 µm) (Figure 2D). The presence of immunotactoid GN in a viral disease confirms the association of immunotactoid GN with a systemic disease, while fibrillary GN is more frequently a 'primary' condition.[71] Fibrillogenesis may be favored by circulating paraproteins interacting with matrix proteins in the glomerulus, such as fibronectin.[72] The animal model of MCGN derived from induction of mixed cryoglobulinemia strongly suggests the pathogenetic role of cryoglobulin rather than a direct etiological role of HCV infection.[73] Of interest, however, and again in the animal model, both RF and cryoglobulinemic properties may be necessary for the development of skin vasculitis, but cryoglobulin activity alone is sufficient to induce glomerular lesions.[74]
| Figure 2. |

{kind=link}
Other uncommon forms of glomerular injury associated with HCV infection include membranous GN, IgA nephropathy, focal and segmental glomerulosclerosis, fibrillary GN, immunotactoid GN rapidly progressive GN, exudative–proliferative GN, and lupus nephritis.[75] Membranous nephropathy in HCV carriers is characterized by absence of cryoglobulin and male predominance.[76]
Treatment
In general, two-stage therapy is considered: removal of cryoglobulins by plasmapheresis and the use of either corticosteroid/cytotoxic agent-mediated immune response attenuation or interferon/ribavirin-mediated viral replication suppression to inhibit their synthesis.
Before HCV and cryoglobulinemic MCGN were discovered to be associated, the mainstay of treatment was corticosteroid and cyclophosphamide. High dose pulse methylprednisolone (1 g/day for 3 consecutive days), followed by oral steroid, were used to control the systemic illness. Plasmapheresis may be applied to remove circulating cryoglobulins, thus preventing their deposition in glomeruli and blood vessel walls. Cyclophosphamide ameliorates the vasculitic injury and inhibits the production of mRFs by B-lymphocytes.[77]
Our current understanding of the association between mixed cryoglobulinemia and HCV infection has allowed a more rational approach to the treatment of this condition. Controlled trials reveal that antiviral therapy with IFN-α improves the systemic symptoms of immune complex disease.[78,79] However, post-therapy relapse occurs in a large proportion of patients, particularly when short-term interferon monotherapy is used. The introduction of combination therapy with IFN-α2b plus ribavirin was an important milestone in chronic hepatitis C treatment,[80] and for the treatment of acute hepatitis C after renal transplantation.[81] Such cocktail therapy has also produced favourable results in mixed cryoglobulinemia, although nonresponses and relapses after initial improvements still occur.[82] In some instances in which sustained viral eradication was unsuccessful, long-term maintenance interferon therapy has led to amelioration of disease. The introduction of pegylated forms of interferon (peginterferon) in the year 2000 represented another breakthrough in the treatment of chronic hepatitis C.[83] Pegylation refers to the covalent attachment of a large inert molecule of polyethylene glycol (PEG) to a protein to yield a molecule that retains biological activity, but has delayed absorption and clearance, allowing for weekly rather than daily or three-times weekly administration. Delayed clearance also led to greater, more potent and longer-lasting antiviral effects. Recent data on peginterferon and ribavirin combination therapy in treating HCV infection are encouraging.[84,85] Furthermore, the higher treatment failure rate of HCV carriers with genotype 1 is recognized.[86] A recent meta-analysis studying 11 clinical trials involving 225 patients revealed that antiviral therapy based on IFN-α can significantly decrease proteinuria and stabilize serum creatinine, and therefore, should be undertaken in patients with HCV-related GN. The improvement in protein excretion is greater in those who achieve HCV RNA clearance, a finding in line with a causal role for HCV in GN.[87]
Despite reports that antiviral therapy can occasionally be associated with a worsening of renal disease or variable response,[88,89] there are increasing numbers of observational studies suggesting the beneficial value of peginterferon and ribavirin combination therapy in treating HCV-related cryoglobulinemic MCGN. A drawback of this therapeutic approach is the complication of hemolysis in ribavirin therapy, especially for patients with renal impairment. This therapeutic issue has been resolved, however, taking glomerular filtration rate into account when determining dosage instead of basing it on body weight alone, as well as administering recombinant erythropoietin to overcome anemia.[90–92] Monitoring the serum ribavirin levels may reduce hemolytic complication, yet serum ribavirin level is not available in most clinical laboratories.[91] Post-treatment renal biopsy showed histological improvement in two of the three patients who received combination therapy for 12 months.[92] In another study in which the viral genotypes were documented, genotype 1 was again associated with a lower sustained VR rate even with combined IFN-α and ribavirin therapy.[93] In severe acute flares of cryoglobulinemia with GN or vasculitis, an appropriate approach is to include corticosteroids and cyclophosphamide as needed to control severe cryoglobulinemic symptoms in addition to combination antiviral therapy. In the most severe cases, plasmapheresis (three to four times weekly exchanges of 3 l of plasma for 2–3 weeks) can be helpful. For refractory cases, monoclonal antibody against the B-cell surface antigen CD20 (rituximab) has been reported to be efficacious with a favorable side-effect profile.[94]
Acute GN Due to Other Hepatitis Viruses
Acute nephritic syndrome complicating fulminating hepatitis A infection is rare. Pathologies including postinfectious GN (endocapillary proliferative GN with low serum complement 3),[95] mesangioproliferative GN with IgM and C3 deposits,[96] and IgA nephropathy[97] have been reported. Spontaneous remission usually occurs with recovery from the hepatitis. GN has not been reported in hepatitis D or hepatitis E.
Chronic hepatitis B and C viral infections are etiologically linked to well-defined glomerulopathies. Renal biopsy with appropriate serological and molecular testing is essential for defining virus-related glomerular lesions and providing prognostic and therapeutic guidance. Antiviral agents remain the mainstay of treatment.
Future Perspective
Chronic HBV and HCV infection remains a major health burden in endemic areas, resulting in hepatic and extrahepatic complications such as glomerulopathy.
For treating HBV-related complications including GN, the future treatment strategy should target: universal vaccination program for endemic areas and populations at risk (such as intravenous drug users); the use of newer antiviral agents, including entecavir, with appropriate dose adjustment according to renal function; stratification of treatment response according to HBV genotype; and downregulation of HBeAg production or enhancement of HBeAg seroconversion through viral mutation as exemplified by precore stop codon mutation and the basal core promoter mutation. For treating HCV-related complications, including GN, the future treatment strategy should target: vaccine development; exploration of the role of the CD4+ T-cell response in the control of early HCV infection, which will increase the opportunity for the identification of protective epitopes that could be used in future vaccine development; stratification of treatment response according to HCV genotype; and clinical trials of newer antiviral agents
Source-Medscape
No comments:
Post a Comment