New Therapies for Chronic Hepatitis C Infection
A Systematic Review of Evidence From Clinical Trials
L. Y. Lee; C. Y. W. Tong; T. Wong; M. Wilkinson
Authors and Disclosures
Posted: 04/13/2012; Int J Clin Pract. 2012;66(4):342-355. © 2012 Blackwell Publishing
Source - Medscape
Abstract
Introduction: Hepatitis C virus (HCV) affects approximately 3% of the world population. The current standard of care for treatment of HCV is a combination of pegylated interferon and ribavirin. Approximately 10% of patients will stop treatment and 30% of patients require dose reduction because of side effects. For genotype 1 HCV-infected patients, only 40% of patients will achieve undetectable viral load 26 weeks posttreatment.
Aims: The objectives of this review were to identify new treatments that are in clinical trials. These include boceprevir and telaprevir which are in routine clinical use and form part of the American Association for the Study of Liver Diseases (AASLD) 2011 guidelines as well as drugs based on observational studies, improving/modifying ribavirin or interferon-based therapies, modifying the host response and finally the use of direct-acting antiviral agents (DAA).
Materials and methods: MEDLINE and EMBASE databases were searched from 2008 to 2011 for treatments for hepatitis C. Furthermore, abstracts and poster presentations for the annual European Association Study of the Liver, AASLD, Digestive Disease Week and Asian Pacific Association for the study of the Liver were searched for relevant material.
Results: All four classes of DAA; NS3/NS4a serine protease inhibitors, cyclophilin inhibitors, NS5b polymerase inhibitors and NS5a inhibitors, show good success rates. Trials have been performed without ribavirin or interferon and demonstrate good antiviral activity with a decreased side effect profile. Combinations of DAA are a promising area of research with a high success rate.
Conclusions: Clinical trials show that future HCV therapy could be personalised, achieve higher success rates with decreased adverse incidents.
Background
Hepatitis C virus (HCV) was only discovered in the 1980s and yet the World Health Organisation estimates that approximately 3% of the world population or 170 million people are chronic carriers.[1] The disease burden of HCV is large with an estimated third of this population likely to progress to liver cirrhosis, of which a third develop hepatocellular carcinoma.
The most common mode of transmission of HCV is exposure to blood products, most commonly from contaminated needles or syringes. The risk of contracting the virus via sexual activity or vertical transmission from mother to child is much lower.
The virus preferentially affects hepatocytes and the acute infection is usually asymptomatic. Most patients fail to clear the virus and become chronic carriers (70–90%). HCV-induced cirrhosis is the second most common cause of liver transplantation in the UK.[2]
The HCV Virion
HCV belongs to the flaviviridae family of viruses and there are six major genotypes of HCV based on analysis of the NS5B regions of the virus.[3]
The virus is an enveloped, spherical single-stranded positive-sense RNA virus. There are two highly conserved untranslated regions (UTR) on either end of the virus genome with the 5' UTR containing the internal ribosomal entry site sequence (IRES).
The genome encodes a polyprotein. The N-terminal consists of the nucleocapsid protein, E1 and E2, and a small ion channel protein, P7. They are followed by the non-structural proteins NS2-NS5, which mediate intracellular aspects of viral functions (Figure 1).

NS2 is initially bound to NS3, but has an autoprotease that splits it into its two constituent halves. NS2 then localises to the endoplasmic reticulum with the envelope glycoproteins.[4]
NS3 is a serine protease that splits the other structural proteins into their active forms. It cleaves NS3-NS4a, NS4a-NS4b, NS4b-NS5a and NS5a-NS5b. It has helicase activity allowing unwinding of double stranded RNA intermediates.[4]
NS4a is a co-factor and helps to anchor the NS3 serine proteases to the intracellular membranes. NS4b induces the formation of a membranous web that becomes the site for HCV replication.
NS5a forms part of the replication complex with NS3-NS5b and has a role in mediating the interferon response (via the secretion of IL8), modulating host-signalling pathways and thus inhibiting apoptosis of infected hepatocytes.[5] NS5b is the viral RNA-dependent RNA polymerase.
Current Therapeutic Targets
Pegylated-interferon and Ribavirin (PEG/RIB) have been the standard of care for treatment of HCV for many years. However, the new AASLD guidelines suggest that the addition of the NS3/NS4a serine protease inhibitors Boceprevir or Telaprevir form 'optimal treatment' for HCV genotype 1 patients.
Interferons are cytokines that are released by host cells in the presence of pathogens. They modulate viral replication, activate other immune cells such as macrophages or NK cells and upregulate antigen presentation via major histocompatibility complex molecules (MHC). Antigen presentation is upregulated by activation of the Interferon-alpha-receptor that results in the transcription of Interferon Stimulated Genes (ISG) via the janus-kinase-STAT signalling pathway.[6]
Since the late 1980s, Interferon has been used for the treatment of hepatitis C. Pegylated interferon (PEG-IFN) was developed in 2001 to enhance the half-life of interferon. There are two types in general use, namely pegylated interferon-alfa-2a and pegylated interferon-alfa-2b, but they are equal in efficacy.[7] They are associated with numerous side effects: 50% of patients experience flu-like symptoms, 25% psychiatric symptoms, 20% symptoms of fatigue or myalgia and 10% symptoms of gastritis/gastroenteritis. Of the psychiatric complaints, 20% of these are severe including acute psychosis, severe depression or personality change.[8]
Ribavirin was developed in 1970 and is effective against HCV when used in combination with interferon. It works by different mechanisms to help suppress HCV infection.[9] The first two mechanisms affect the host response:
- It is immunomodulatory and enhances Th1 CD4 responses resulting in increased activity of cytotoxic T lymphocytes and secretion of antiviral cytokines such as interferon-γ and TNF-α.
- It upregulates the host interferon-stimulated genes that have roles in combating viruses by upregulating the interferon alpha receptor and downregulating the interferon inhibitory pathways.
- The final three mechanisms target the HCV:
- It stops viral replication by inhibiting the formation of the guanosine nucleoside by inhibiting IMPDH (inosine monophosphatase dehydrogenase).
- It inhibits the NS5B RNA dependent RNA polymerase.
- It induces lethal mutagenesis by increasing errors in translation of E2, NS5A and NS5B.
When used in combination, approximately 10% of patients will withdraw from therapy because of adverse events and 32% of patients will require a decrease in dose, which reduces the effectiveness of the PEG/RIB.[13]
Reasonable rates of Sustained Virological Response, defined as undetectable viral load 26 weeks following the end of treatment, i.e. a cure, can be achieved with PEG/RIB. Sustained virological response (SVR) rates are 38–41% for genotype 1,[7] 93% for genotype 2, 79% for genotype 3[14] and 69% for genotype 4.[15] Treatment duration can be shortened depending on the presence or absence of undetectable HCV RNA at week 4 (Rapid Virological Response, RVR)[16] and according to the genotype of the HCV.
Patients with different polymorphisms in the IL28B host gene have different rates of SVR. Thus, patients with the IL28B rs12979860 CC genotype have a twofold higher SVR rate than those with the T allele.[17] However, IL28B is less important in genotypes 2 and 3 HCV-infected patients.[18]
New Therapies
Over 40 new treatment options are undergoing clinical trials for the treatment of HCV.
Current research is aimed at four major areas;
- Using medications Based on Observational Studies.
- Improving and modifying ribavirin or interferon-based therapies.
- Modifying host response.
- Development and use of direct-acting antiviral agents (DAA).
Methods
Search Strategy
Relevant studies and abstracts were obtained by searching MEDLINE (1948 to July 2011) and EMBASE (1980 to July 2011). There was no language restriction and the initial search strategy was developed from the search headings 'liver disease' and 'clinical trial' removing references to 'hepatitis B', 'hepatitis A', 'autoimmune' or 'alcohol'. A further search was done for the term 'antiviral' or 'antivirus agent' or 'antiviral activity' and 'clinical trial'. These searches were limited from January 2008 to July 2011. Abstracts and poster presentations from the annual European Association Study of the Liver, AASLD, Digestive Disease Week and Asian Pacific Association for the study of the Liver were searched for relevant material for the same time period. In addition, the reference lists from the retrieved papers were hand searched.
Selection Criteria (Figure 2)

Studies were included if they[1] included an adult population (age > 18 years);[2] had a serological diagnosis of HCV;[3] had an intervention and[4] had an outcome measure. This could either be an SVR, Early Virological Response (Undetectable HCV RNA at week 12), Rapid Virological response (undetectable HCV RNA at week 4) or rate of fall of HCV RNA levels. Studies were excluded if patients were co-infected with other viruses such as HIV or HBV.
Data Extraction
A spreadsheet was created that recorded study characteristics including authors, study title, sample size, publication year, type of intervention, name of drug, whether the drug was used with PEG/RIB or as monotherapy. Patient characteristics were recorded such as genotype, if the patient was treatment naïve or experienced and ethnicity (if relevant). The study results were measured by looking at percentage of patients with rapid virological response (RVR- undetectable HCV RNA at week 4), early virological response (EVR- undetectable HCV RNA at week 12) or sustained virological response (SVR- undetectable HCV RNA 12 weeks after treatment), rate of fall of HCV RNA levels, notable side effects and conclusions.
Results
Medications based on observational studies (Table 1)
Patients with impaired glycaemic control treated with PEG/RIB have much lower rates of SVR.[19] A number of investigators have looked at lipid-lowering agents to see if they could improve clinical response to PEG/RIB.
The addition of simvastatin, ezetimibe, fluvastatin, rosuvastatin and pioglitazone has all been noted to improve the anti-viral activity of PEG/RIB.[20–23] Non-steroidal anti-inflammatory drugs also have the ability to potentiate interferon signalling and ketoprofen increases SVR rates marginally.[24] However, as the additional anti-viral effects are minimal, these drugs are not used as adjuncts to PEG/RIB Table 1.
Ribavirin or Interferon-type Analogues
Ribavirin Analogues
These derivatives aim to reduce the anaemia that is associated with ribavirin therapy.
Taribavirin is a ribavirin prodrug with a similar spectrum of antiviral activity, but with better hepatocyte specificity and less accumulation in erythrocytes. An amidine group inhibits taribavirin drug entry into erythrocytes and this causes less anaemia.
Two randomised controlled studies showed no statistical difference in SVR rates between taribavirin and ribavirin, but a lower incidence of anaemia (13.4% vs. 32.9%).[25] Unfortunately, poorer results were noted in the larger ViSER2 study. The ViSER2 study was the phase 3 study and noted that whilst taribavirin did cause less anaemia, non-inferiority was not achieved.[26]
Interferon Analogues (Table 2)
Interferon has inherent limitations. It has a short half-life because of its small size, susceptibility to serum proteases and rapid renal clearance. Six new interferon-type therapies have been developed to treat HCV Table 2.
Interferon-α-2B-XL and omega interferon demonstrated a better side effect profile than pegylated interferon.[27]
Fortnightly interferons have been developed such as Albinterferon (albuferon−, Human Genome Sciences, Rockville, MD, USA) and CR2b (Locteron−/BLX-883, Octoplus, Leiden, the Netherlands). Prolonged release of interferon is associated with fewer side effects than traditional interferons because of the lower initial peak of interferon concentrations. Albinterferon consists of interferon alpha linked to human albumin.
A phase 2 study looked at Albinterferon use in prior non-responders, a group of patients with poorer treatment success rates. It noted that there was a lower incidence of adverse incidents with similar SVR rate compared with Pegylated interferon.[28] Phase 3 randomised controlled trials using Albinterferon in genotypes 1, 2 and 3 have all shown non-inferiority with a similar SE profile.[29]
The EMPOWER trial and SELECT-2 trials noted that CR2b not only achieved non-inferiority but also reduced flu symptoms by 50%.[30,31]
PEG-Interferon lambda 1 (IL-29) is a new class of interferon that binds to a different receptor to PEG-IFN-α. The receptor for interferon lambda is more hepatocyte-specific and thus has the potential for an improved side effect profile. The results from the recent Phase 2b EMERGE clinical trial showed that PEG-interferon lambda achieved higher rates of RVR in genotypes 1, 2, 3 and 4. In addition, there was a decrease in flu symptoms (9.7–12.5% vs. 42.9%), musculoskeletal symptoms (14.2–18% vs. 46.6%), anaemia with Hb <10 g/dl (12.9–20.5% vs. 43.9%) and thrombocytopaenia (0% vs. 14.4%). There was also less need for dose reductions.[32
Modification of the Host Response
This can be achieved by three means: vaccines that target the conserved areas of the HCV genome, direct immunomodulators that improve interferon signalling and matrix metalloprotease inhibitors that inhibit viral spread.
Vaccinations (Table 3)
Hepatitis C has a high mutation rate. Most mutations occur around the area of the genome coding for the envelope protein (E2) that allows the virus to evade the immune system. The development of vaccines has been problematic because each patient has a different mix of viral proteins and these vary from patient to patient as well as at different periods of time. Vaccines are aimed at highly conserved parts of the virus, such as the NS3/NS4a core protein (GI 5005 or ChronVac-C) or at a large number of highly conserved non-structural proteins such as NS3/NS4 and NS5b (TG4040) Table 3.
Only three vaccines have some success in clinical trials: TG4040, GI5005 and ChronVas-C− (Chrontech pharma AB, Huddinge, Sweden).
The vaccines TG4040 and ChronVac-C− vaccines express NS3/NS4A genes with a modified vaccinia virus or a cytomegalovirus promoter. These drugs cause a transient decrease in viral load.[33]
The vaccine GI5005 is in the furthest stage of development. It is a recombinant saccharomyces cerevisiae that expresses NS3 and core proteins. In treatment-naïve patients treated with GI 5005 and PEG/RIB for 48 weeks compared with PEG/RIB, the SVR rate was 74% vs. 58%. In previous treatment non-responders, the SVR rate was increased to 63% from 47%. There was no increase in adverse effects.[34]
Immunomodulatory Agents (Table 4)
Direct immunomodulators exert antiviral actions by improving interferon signalling [EMZ702,[35] S-adenosylmethionine[36] and Nitazoxanide[37]], T-cell responses (Thymosin and SCV-07) or protecting lymphocytes from apoptosis (histamine dihydrochloride) Table 4.
EMZ702 enhances the action of interferon. A trial with EMZ702 combined with PEG/RIB showed that EVR could be increased to 28% in previous non-responders.[35] However, further research has been discontinued.
S-adenosyl methionine (SAMe) also acts by improving interferon signalling. SAMe + PEG/RIB improves rates of viral decline and EVR.[38]
Nitazoxanide was originally developed as an antiparasitic drug, but was subsequently found to augment interferon. In a study looking at genotype 4 HCV patients treated with nitazoxanide with PEG/RIB vs. PEG/RIB, rates of RVR and SVR were increased without an increase in adverse side effects.[37]
Thymosin and SCV-07 are both immunomodulators that augment T-cell responses. When Thymosin was used with interferon, SVR rates were increased.[39] This is also the case in chronic HCV non-responders.[40]
There has only been one small phase 1 trial for SCV-07, in which it resulted in good reductions in HCV viral load.[41]
Histamine dihydrochloride potentiates the IFN-alpha induced activation of T cells by protecting these lymphocytes against oxygen radicals and thus preventing apoptosis. When given with interferon, rates of SVR ranged from 37% to 44%.[42]
Matrix Metalloprotease Inhibitors (MMPI)
The final method of modifying the host response is via matrix metalloprotease inhibitors. Matrix metalloproteases (MMP) are host proteins that degrade the extracellular matrix. HCV viral proteases upregulate MMP and this facilitates viral spread.
CTS-1027 is a molecule that inhibits MMP activity. CTS-1027 was given with ribavirin to genotype 1 treatment-naïve patients. The trial showed modest reductions in HCV RNA at 24 weeks.[43] When CTS-1027 was combined with PEG/RIB in non-responders, the virological response was increased at 24 weeks compared with historical controls.[44]
Direct-acting Antiviral Agents
With the exception of Boceprevir and Telaprevir, direct-acting antiviral agents (DAA) are in early stages of development. When used as monotherapy, they pose a high risk for the selection of resistant mutants. Monotherapy with new DAA agents has been limited to short-term therapy and most research focuses on combinations of the new DAA with PEG/RIB. However, within the last two years, the most exciting research aims to minimise side effects by using combinations of DAA without interferon or ribavirin.
There are four classes of DAA: NS3/NS4a serine protease inhibitors, cyclophilin inhibitors, NS5b polymerase inhibitors that inhibit the RNA-dependent RNA polymerase and NS5a inhibitors that disrupt signalling and the replication complex.
NS3/NS4a Serine Protease Inhibitors (Table 5)
HCV requires a highly-conserved serine protease to split the other structural proteins into their active forms. A large number of drugs have been developed to target this enzyme, two of which, telaprevir and boceprevir, have completed phase 3 clinical trials. Telaprevir and boceprevir now form 'optimal therapy' for chronic HCV genotype 1 infection in the recently published AASLD guidelines 2011 and are in routine clinical practice Table 5.
The benefits of telaprevir +PEG/RIB over PEG/RIB have been demonstrated in the PROVE 1 + 2 trials[45] and the ADVANCE trials.[46] Telaprevir increased SVR up to 75–92% compared to 44% with PEG/RIB. Unfortunately, treatment was associated with a severe rash and anaemia that led to treatment discontinuation in 8% and 3% of patients, respectively.
The benefits of boceprevir + PEG/RIB over PEG/RIB were demonstrated in the SPRINT-2 trial,[47] with SVR rates increased to 63–66%. However, anaemia and dysgeusia are prominent side effects in 50% and 40% of patients, respectively. Whilst there was no increase in discontinuation rates, almost double the patients required erythropoietin use or dose modification compared with PEG/RIB.
Further studies with telaprevir and Boceprevir noted that rates of SVR were independent of IL28B genotypes.[48] However, a cost-modelling exercise noted that a CC IL28B polymorphism might make treatment less cost-effective.[49] Treatment could be shortened depending on early response.[50] Both drugs are beneficial in patients who have previously failed treatment (EXTEND and RESPOND-2 trials).[51] Follow-up studies for up to three years have noted that SVR rates are durable.[52] Studies have also shown good decreases in viral load when using telaprevir and boceprevir monotherapy in genotypes 2 + 3 patients.[53,54]
There are a number of other drugs in this field. ACH-1625,[55] GS-9256,[56] Narlaprevir,[57] SCH-900518[58] and IDX 184[59] result in decreases in viral load. ABT 450[60] and BMS650032[61] result in significantly higher EVR and RVR rates.
Trials for MK7009,[62] RG7227[63] and TMC435[64] used with PEG/RIB have all shown increased rates of SVR. TMC435 has also been shown to be effective in patients who have had previous treatment failure.[65]
Of these new drugs, BMS650032 and MK7009 have a smaller side effect profile than telaprevir and boceprevir. Mutational analysis has noted that certain mutations have been linked to poor response, such as R155K and D168V in ABT-450.
Cyclophilin Inhibitors (Table 6)
Cyclophilin is a host protein that is a co-factor required for assembly of the HCV replication complex together with NS5B. As cyclophilin inhibitors act on host proteins unlike other DAA, it is expected that they will have better antiviral activity against all genotypes. Three cyclophilin inhibitors have entered clinical trials Table 6.
Monotherapy with SCY-635 and NIM811 induces consistent decreases in viral load when given for 15 days and 8 days, respectively, with no increase in adverse effects.[66]
Debio-025 is at a further stage of clinical development. When used with pegylated interferon, a good RVR of 67% with a mild side effect profile has been achieved.[67]
NS5B Polymerase Inhibitors
The RNA-dependent RNA polymerase NS5B is responsible for translation of the HCV RNA template. NS5B can be inhibited in two ways. Analogues of naturally occurring deoxynucleotides may be used. Nucleotide polymerase inhibitors (NPI) compete with the natural deoxynucleotides for incorporation, but when added, they terminate the growing RNA chain and result in incomplete translation (Figure 3).

Figure 3.
Mechanism of action of NS5B nucleotide polymerase inhibitors.
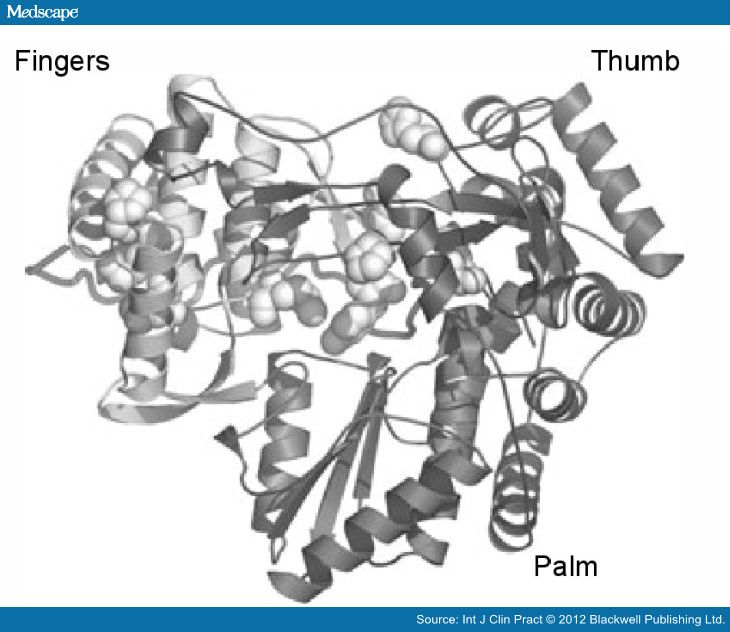
Figure 4.
Structure of HCV NS5B RNA dependent RNA polymerase.
Nucleotide Polymerase Inhibitors-NPI (Table 7)
There have been four successful clinical trials involving IDX184, PSI 7977, R1626 and RG7128 Table 7.
R1626 demonstrated good antiviral effects as monotherapy[68] and in combination with IFN.[69] However, concerns about neutropenia have halted further clinical trials.
PSI-7977 and IDX184 have shown promising results in monotherapy.[70] Phase 2 trials have noted that both cause a significant increase in rates of viral suppression when used for short durations of 28 and 14 days. SVR rates for PSI-7977 when combined with ribavirin was 100% for genotype 2 and 3 patients[71]
The PROPEL trial looking at RG7128 is the largest clinical trial. EVR was increased significantly from 49% using PEG/RIB to 80–88% with a RG7128/PEG/RIB combination. There was no increase in adverse events.
Non-Nucleotide Polymerase Inhibitors-NNPI (Table 8)
Non-nucleotide polymerase inhibitors bind to NS5B polymerase active sites Table 8.
Silibinin is the active constituent of silymarin, a herbal remedy for hepatitis extracted from milk thistle. IV silibinin is able to reduce viral load,[72] but there was no effect on SVR when used with PEG/RIB.[73] BILB-1941, MK3281, VCH759 and VX222 used in monotherapy have shown good anti-viral properties, although in the case of BILB-1941 its development has been limited by side effects.[74–76]
BI207127,[77] Filibuvir,[78] ANA598,[79] ABT-072 and ABT-333 have good antiviral properties. When used with PEG/RIB, BI207127 increased rates of RVR,[80] ABT-072, ABT-333[81] and filibuvir achieved high rates of EVR. However, ANA598 treatment with PEG/RIB did not have any advantage over PEG/RIB.[82]
Interestingly, mutational analysis was performed for HCV patients treated with filibuvir. A poor response to filibuvir was associated with a M423T/V mutation.[83] In future mutational analysis will be used to select the drug with the best SVR for that patient.
However, whilst it is extremely promising that the majority of the NPIs increase rates of EVR and RVR, caution should be heeded as EVR/RVR does not necessarily lead to improvements in rates of SVR. Treatment with GS9190 + PEG/RIB increased the rates of EVR, but not that of SVR.[78]
NS5a (Table 9) NS5a forms the replication complex with NS3-NS5b and has a role in mediating interferon responses and inhibiting apoptosis.[5] There are currently two inhibitors in clinical trials, BMS824393 and BMS790052 Table 9.
BMS824393 has good results when used as monotherapy.[84] BMS790052 combined with PEG/RIB significantly improves rates of SVR to 92% from 25% with a similar side effect profile.[85]
Combinations of Direct-acting Antiviral Agents
The principle of combining DAA is based on the human immunodeficiency virus (HIV) treatment paradigm, although unlike HIV, treatment for HCV only requires a finite duration of treatment and is curative. The principle is that combinations of drugs that target different steps of viral replication can decrease rates of viral resistance and increase rates of viral suppression.
The first combination clinical trial (INFORM-1) looked at a combination of a nucleotide polymerase inhibitor, RG7128, and a NS3/NS4b protease inhibitor, RG7227 + PEG/RIB. The trial noted high rates of EVR compared with PEG/RIB and this combination achieved profound antiviral suppression greater than monotherapy.[86]
The Nuclear study looked at combinations of a pyrimidine analogue (PSI-7977) and a purine analogue (PSI-938) without PEG/RIB. At week 2, 88–100% of patients had undetectable viral loads.[87] In addition to demonstrating that two nucleotide polymerase inhibitors could be used in combination successfully, this was one of the first studies that demonstrated the feasibility of Ribavirin- and interferon-free treatments.
A further interferon free combination of the NS3/NS4a protease inhibitor, BI201335 and the non-nucleotide polymerase inhibitor, BI207127 in conjunction with ribavirin produced 100% RVR.[88]
In the last year, two studies have stood out as particularly promising as they reinforce the notion that interferon and ribavirin, whilst efficacious, may not be necessary to reduce HCV viral load to undetectable levels.
The NS3/NS4a serine protease inhibitor (GS9256) and a non-nucleotide polymerase inhibitor (GS9190) were used in combination with and without ribavirin in genotype 1 treatment-naïve patients. At week 12, GS-9256/GS9190 combinations produced an EVR rate of 80% (n = 15) that was increased to 100% when ribavirin was added (n = 13).[89]
The second study combined the NS3/NS4a serine protease inhibitor (BMS-650032) with an NS5a (BMS-790052) in patients with previous treatment failure. A good SVR rate of 90% was obtained. Resistance to BMS-790052 is associated with polymorphisms associated with L28M, R30Q, L31M and Y93H.[90] When quadruple therapy with BMS-650032/BMS-790052/PEG/RIB was used for 10 treatment non-responders with genotype 1, 100% SVR was obtained.
Conclusions
Interferon and Ribavirin have been used as the gold standard for treatment of hepatitis C. However, there are relatively low success rates and significant side effects with a large proportion of patients requiring dose reduction or discontinuing treatment.
Concurrent therapy with drugs such as simvastatin can increase rates of SVR modestly. However, newer drugs have the potential to increase rates of SVR significantly.
Newer interferons and ribavirin analogues have been developed that allow decreased frequency of dosing, decreased side effect profiles and lower rates of anaemia. The most promising drug is albinterferon, which is in phase 3 trials.
Vaccines, immunomodulator drugs and matrix-metalloproteases inhibitors are targeted at the host responses. The vaccine GI5005 + PEG/RIB increases rates of SVR in HCV-infected patients and further trials looking at prevention of infection would be of interest.
DAAs are exciting new treatments that target NS3/NS4a serine proteases, cyclophilins, NS5a or the NS5b polymerase. Telaprevir and boceprevir significantly improve SVR rates to over 70%, albeit with an increased side effect profile. Beyond telaprevir and boceprevir, newer DAAs are in development that have reduced frequency of dosing, decreased side effects and higher efficacy, such as the NS3/NS4a drug TMC 435/BI201335 or the Nucleotide polymerase inhibitors, PSI-7977.
Combinations of DAAs show much promise. The concept of treatment of HCV without ribavirin or interferon is novel, but trials show that combinations have good antiviral effects with a much lower side effect profile compared with PEG/RIB. Furthermore, if interferon and ribavirin were combined with combinations of DAA such as BMS-650032 and BMS-790052, nearly 100% of patients may achieve SVR.
However, most trials are only in phases 1/2 and considerable research is required to show which combinations of drugs will be effective. In addition, most of the HCV research has been in genotype 1 naïve HCV patients and thus is not applicable to all HCV patients. More research is required for patients infected with genotype 2–6 and those with previous treatment failures.
In the future, the field of mutational analysis of the HCV genome will play an important role. Trials have demonstrated that this strategy is able to predict poor responses, e.g. the M423T mutation and treatment with filibuvir. In the future, clinicians may perform routine mutational analysis of the HCV genome and select the best combination of drug accordingly.
The next decade looks exciting for HCV research. Over 40 drugs acting via a multitude of different mechanisms are undergoing clinical trials. It is hoped that personalised HCV therapy achieving high success rates but minimal side effects may soon be achievable.
No comments:
Post a Comment