Posted: 05/19/2011; J Viral Hepat. 2011;18(4):e99-e103. © 2011 Blackwell Publishing
Extended Treatment Duration for Treatment Naïve Chronic Hepatitis C Genotype 1 Late Viral Responders
A Meta-analysis Comparing 48 Weeks vs 72 Weeks of Pegylated Interferon and Ribavirin
Abstract and Introduction
Patients with genotype I chronic hepatitis C virus (HCV) infection with late virological response to therapy have low sustained viral response (SVR) with standard 48 weeks of therapy and may benefit from extended therapy. We performed a systematic review and meta-analysis of five studies to compare the outcome of 48 weeks vs 72 weeks treatment in treatment naïve chronic hepatitis C genotype I patients with late virological response. The end of treatment response with extended 72 weeks of treatment compared to standard 48 weeks of treatment was similar 48% and 56%, respectively, with pooled odds ratio (OR) (0.85; 95% CI 0.52–1.37). However, the SVR rates were higher with 72 weeks of treatment compared to 48 weeks treatment 32%vs 25% with pooled OR of 1.67 in favour of extended duration therapy (95% CI 1.16–2.40). This was because of lower relapse rates with extended duration therapy (35%vs 55%) with OR of 0.39 in favour of 72 weeks therapy (95% CI 0.25–0.61). There was no heterogeneity. No publication bias was noted as assessed by Egger's test. Extending the treatment duration from 48 to 72 weeks in genotype 1 infected patients with late virological response improves SVR. Thus, therapy extension in genotype 1 late viral responders (LVR) may be a consideration to improve treatment response; however, the proportion of patients with LVR that might benefit from 72-week therapy appears to be small.
Introduction
An estimated 170 million individuals are infected with hepatitis C virus (HCV) worldwide.[1] Eradication of the virus in infected individuals is imperative to avoid long-term-related complications of cirrhosis, decompensated liver disease and hepatocellular carcinoma. Current treatment strategies with combination pegylated interferon and ribavirin are suboptimal and are dependent on a number of host factors, viral factors and treatment factors. Overall, 56% of HCV patients achieve sustained virological response (SVR), and patients with genotype I infection achieve even lower rates of SVR.[2] Recently, some authors have suggested on-treatment viral kinetic responses are more predictive than pretreatment factors for SVR.[3] Treatment response-guided therapy may maximize SVR and minimize costs and adverse events of therapy.
The current treatment duration for HCV genotype I infected patients is 48 weeks of combination pegylated interferon and ribavirin. Patients with rapid virological response (RVR), defined as undetectable serum HCV at week 4, achieve high rates of SVR up to 87% on this therapy. Patients with early virological response (EVR), defined as <2-log drop in serum HCV at week 12, achieve 27–68% rates of SVR.[2–6] Therapy is discontinued in patients who do not achieve EVR because of SVR rates of only 5%. With availability of more sensitive serum HCV RNA methods, a distinction has been made between complete EVR, defined as undetectable HCV RNA at week 12, with SVR up to 68% and partial early virological response (pEVR), defined as detectable but >2 log drop in serum HCV RNA, with SVR up to 43%. Furthermore, patients with pEVR can also be categorized as late viral responders (LVR) if serum HCV RNA is undetectable at week 24.[2–6] Recent randomized controlled trials (RCTs) suggest that patients with LVR with extended duration of therapy to 72 weeks achieve higher rates of SVR than standard 48 weeks of therapy.[7–12] However, the difference has not been statistically significant in all the trials.[10,11] The lack of significance may be related to small sizes, resulting in a lack of power for detecting clinically meaningful differences. In this study, we undertook a systematic review of the literature and performed a meta-analysis to compare 72 weeks of treatment to the standard duration of 48 weeks in HCV genotype I patients with LVR.
Methods
Literature Search
Three independent investigators (MP, AS and GS) searched the electronic data base literature (Medline, Cochrane Reviews, and EMBASE, ISI Web of science) from 2004 to 2010 for all types of publications including abstracts. The search terms used were hepatitis C, HCV, pegylated interferon, ribavirin, genotype 1, slow virological response, late virological response and extended therapy. Boolean logic was used to combine the words. In addition, a manual search was performed for cross-references from publications reviewed.Study Selection
Criteria for study selection Three independent reviewers (MP, AS and GS) selected the studies to analyse the effect of extending treatment duration to 72 weeks in treatment naïve chronic hepatitis C genotype 1 infected patients with LVR using the following criteria: (i) study design – RCT; (ii) study population – genotype 1 HCV treatment naïve patients achieving LVR; (iii) treatment – pegylated interferon and ribavirin combination; (iv) treatment duration – comparing standard 48 weeks treatment and extended duration 72 weeks treatment; (v) definition of LVR: greater than 50 IU/mL or at least a 2 log decrease but detectable HCV RNA at week 12 and undetectable HCV RNA at week 24.
Outcome measures
Outcome measures were end of treatment response (ETR), sustained virological response and relapse rates (RR).
Assessment of Study Quality
Three independent reviewers (MP, AS and GS) assessed the study quality. Any conflict of the reviewers was resolved by consensus. Studies were graded using the Jadad criteria.[13] These criteria include three methodological features of randomization, blinding and accountability of all patients. Each study was given a numerical score in the range 0–5. A higher score provided a stronger measure of study design and quality. One point was scored for each of the following: (i) study described as randomized; (ii) method used to generate the sequence of randomization described and appropriate; (iii) study described as double blind; (iv) method of double blinding described and appropriate; (v) description of withdrawals and dropouts.[13]
Data Collection
Data were extracted by the three researchers (MP, AS and GS) independently and cross-checked for completeness and accuracy. Data were collected on country(ies) of study, sample size, duration of treatment, pegylated interferon type and weekly dose, ribavirin daily dose, method of detection of HCV viral load, definition of LVR, ETR, sustained virological response (SVR), RR and discontinuation rates if available.Data Analysis and Statistical Methods
Data were entered into the software (Revman 5) adding one study at a time. The odds ratio (OR) was used as a member of association. After adding data from all the studies, summary OR with 95% confidence interval (CI) and Forrest plot graphs were obtained. Study heterogeneity was obtained to assess whether the treatment effect variation across the studies was significant (χ2 P < 0.1) rather than one expected by chance. To take the effect of heterogeneity into consideration, DerSimonian and Laird random effects model was used for analysis. Publication bias was investigated through visual inspection of funnel plots and using the Egger test. Sensitivity analysis was performed after excluding studies with the highest and lowest ORs.
Selection of Studies
The literature search and selection flow process is shown in Fig. 1. After initial screening, 10 relevant studies were selected. After applying the inclusion criteria, only five studies[7,9–12] were available to analyse the effect of extended treatment duration for treatment naïve chronic hepatitis C genotype 1 patients with late virological response with pegylated interferon and ribavirin. Five studies were excluded for the following reasons: two retrospective studies,[14,15] one failed to mention a study design,[16] one lacked a control group[17] and one utilized an alternative definition of late virological response.[8]
Click To Enlarge Figure One
Click To Enlarge Figure One

Figure 1
Literature search and study selection process
Study Characteristics
Literature search and study selection process
Study Characteristics
The characteristics of the studies are shown in Table 1. All five studies were published as original articles. Two RCTs[7,10] compared outcome measures of treatment duration of LVR through retrospective subgroup analysis. One study included genotype 4 patients.[12] All studies were conducted in Western countries. The sample size varied from 74 (10) to 206 (7). Both pegylated interferon types alpha 2a and alpha 2b were used. Ribavirin daily dose ranged from 800 mg up to 1400 mg per day.
Quantitative Analysis
End of Treatment Response Quantitative Analysis
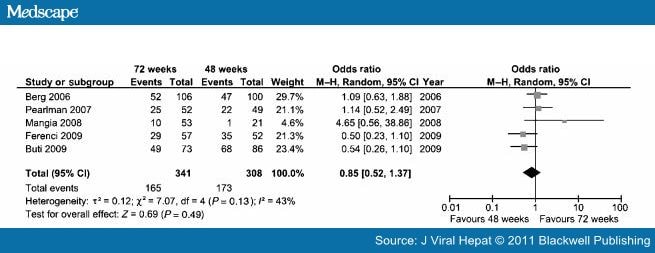
The pooled data from the five studies showed an ETR of 56% with standard 48 weeks and 48% with extended 72 weeks of treatment, with pooled OR (95% CI) of 0.85 (0.52–1.37). There was no significant difference in the ETR between the two groups (P = 0.49) (Fig. 2). There was mild heterogeneity (I 2 = 43%).
Click On Figure To Enlarge
{kind=link}
Forest plot for end of treatment response comparing 72 weeks vs 48 weeks of pegylated interferon and ribavirin treatment.
Sustained Virological Response
The pooled data from the five studies showed an SVR of 25% with 48 weeks of treatment and 32% with 72 weeks of treatment. The OR (95% CI) for SVR was 1.67 (1.16–2.40) in favour of extended duration treatment. The difference was significant (P = 0.006) (Fig. 3). The data were homogenous (I 2 = 0%).
Click On Figure To Enlarge
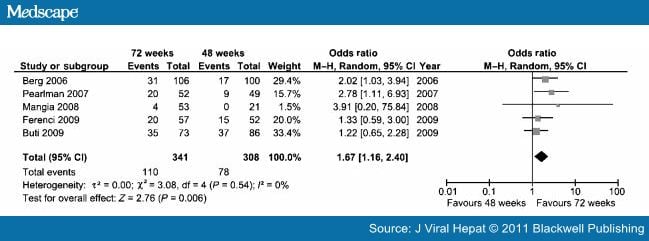
Figure 3.
Forest plot for sustained virological response comparing 72 weeks vs 48 weeks of pegylated interferon and ribavirin treatment.
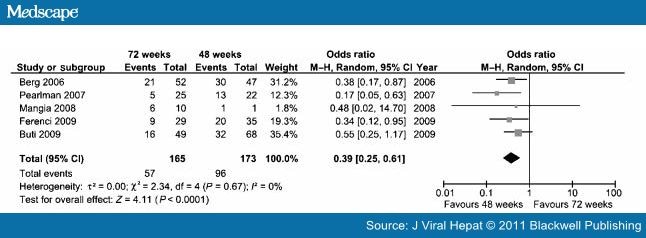
Relapse Rates The pooled data from the five studies showed RR of 55% with 48 weeks of treatment and 35% with 72 weeks of treatment. The OR (95% CI) for RR was 0.39 (0.25–0.61) in favour of 72 weeks of therapy with P-value < 0.0001 (Fig. 4). The data were homogenous (I 2 = 0%).
Click On Figure To Enlarge
.
Figure 4
Forest plot for relapse rates comparing 72 weeks vs 48 weeks of pegylated interferon and ribavirin treatment.
.
Disscussion
The pooled data from this meta-analysis showed that in LVR, the SVR rate was higher with extended 72 weeks of treatment compared to 48 weeks of treatment. However, the ETR was not different in the two groups. The high SVR rates were because of lower RR with extended duration therapy (35%vs 55%).
Should we recommend 72 weeks of pegylated interferon and ribavirin for patients who are slow to clear HCV RNA? This meta-analysis provides pooled data from well-conducted quality randomized controlled studies including prospective follow-up of treatment in three studies. The result of this meta-analysis suggests benefit of extended therapy in this group of patients with chronic HCV infection. Although statistically significant, the difference in favour of extended duration therapy in patients with LVR is still rather small. There is also some concern regarding compliance and tolerance of extended therapy. Although discontinuation rates were not reported in all the studies, overall extended therapy had higher discontinuation rates compared to standard treatment (20%vs 11%). Higher discontinuation rates appeared to be secondary to higher rates of voluntary withdrawal rather than serious adverse events from prolonged therapy. Therefore, it seems the risk of adverse events is similar between standard and extended duration of therapy and patient compliance would be the issue with extended therapy.
There are some limitations to this analysis. Berg et al. [7] used a suboptimal fixed dose of ribavirin 800 mg per day compared to the standard weight–based ribavirin 1000–1200 mg per day for genotype 1 infection.[6] This differential dosing may have accounted for the difference in SVR and RR between 48 and 72 weeks. If standard weight–based ribavirin was administered, then perhaps the SVR rates would have been higher in the 48 weeks treatment group. In addition, dose reductions were permitted throughout all the studies. There was no uniformity among studies for use of growth factors. Lastly, two studies[7,10] used subgroup analysis to compare outcome measures upon trial completion. Another concern has been which definition of nonresponse should be used. Few studies have used failure to achieve undetectable HCV RNA at 4 weeks (non-RVR) as criteria for extension of treatment. Recently, it has become clearer that RVR is better suited to predict success with short duration of treatment, and virological testing at 12 weeks is preferred time to select patients for extended duration. In our analysis, we excluded the studies using 4 weeks nonresponse as a guide to extended therapy.
The development of specifically targeted antiviral therapy for hepatitis C (STAT-C) is rapidly advancing and with advent of newer therapies for hepatitis C, it is unlikely future studies will address the benefit of extended therapy. It is expected that studies of newer protease or polymerase inhibitors will show higher response rates in this group of patients. Unlike the current therapies, the protease inhibitors are susceptible to developing various resistance patterns.[18] Although extended therapy is more expensive than standard therapy, extended therapy may be more cost-effective compared to newer STAT-C therapies.
In conclusion, extending the treatment duration from 48 to 72 weeks in genotype 1 infected patients with late virological response improves SVR rates because of lower RR. Thus, therapy extension in genotype 1 LVR may be a consideration to improve treatment response; however, the proportion of patients with LVR that might benefit from 72-week therapy appears to be small.
No comments:
Post a Comment