 Bakers Union Marching Through the Labor Day Parade
Bakers Union Marching Through the Labor Day Parade
What's Hot in September/October 2011
by David W. Sharp
In just seven weeks between the beginning of June 2011 and mid-July appeared at least 20 research papers on a single-nucleotide polymorphism (SNP) lying on chromosome 19 close to the gene (IL28B) that encodes a type III interferon. This is an astonishing rate of publication, a trigger for which must surely have been the contribution now standing at #6 in the Top Ten, with an accumulated 279 citations in the Hot Papers database as of March-April 2011.
This publication showed that genetic variation in IL28B can help clinicians and patients predict response to treatment (pegylated interferon and ribavirin being the current standard) given for
hepatitis C. A companion paper now stands at #25 (D.L. Thomas, et al., Nature, 461[7265]: 798-801, 2009; total cites 160, latest count 43), this being concerned with the natural history of hepatitis C, whereas the report from three weeks earlier in 2009 (#6) looked at sustained viral clearance in response to treatment.
The SNP, known as rs12979860, was identified via a genome-wide association study. Genetic markers like this need confirmation, and for rs12979860 and hepatitis C this came rapidly and consistently. For example, a statistical exercise revealed genotype CC to be the strongest predictor of response to antiviral treatment (T.R. O’Brien, et al., PLoS One, 6[7]: e20904, 2011 [Epub July 8, 2011]). The genotyping can now be done rapidly (e.g., R. Melis R, et al., J. Mol. Diag., 13[4]: 446-51, 2011), and within a year of the seminal publication the case was being made for IL28B genotyping being built into the design for trials of hepatitis C treatments.

DNA molecule 1 differs from DNA molecule 2 at a single base-pair location (a C/T polymorphism),
Wiki Commons.
The previous Top Ten commentary in
July/August 2011touched on a new drug for melanoma (vemurafenib or PLX4032) which had attracted attention at an oncology meeting earlier this year. The topic deserves more space because at #11 this time we have a phase I study of this drug (K.T. Flaherty, et al., New Engl. J. Med.,363[9]: 809-19, 2010; total cites 116, latest count 62).
Roughly half of all melanomas carry a mutation in the gene that codes for a kinase called BRAF, and vemurafenib is a powerful inhibitor of BRAF with this mutation. At least three other drugs with the same target are being looked at. Although the study focused on drug dosage and toxicity, encouraging tumor responses were recorded. A phase III clinical trial was reported to be in progress—indeed, we now have the six-month results from that (P.B. Chapman, et al., New Engl. J. Med., 364[26]: 2507-16, 2011).
Six hundred and seventy-five patients with previously untreated metastatic melanoma and possessing the specific mutation took part in this randomized comparison of vemurafenib and dacarbazine. Overall survival was 84% for patients on the new drug and 64% for the control group, and the trial monitoring committee advised switching those on dacarbazine to vemurafenib. Drug approval is being sought from U.S. and European licensing agencies, and a rapid diagnostic test for the mutation has been developed.
If vemurafenib does prove to be the breakthrough that we all hope for, this will provide huge encouragement to everyone involved in the development of genetically tailored cancer treatments, where there have been so many ups and downs. Vemurafenib itself is no exception to this "roller coaster of breakthroughs and setbacks" (as recorded in Amy Harmon’s New York Times series on this drug in February, 2010).
This development has involved basic-research companies and the pharmaceutical industry working together—indeed, Roche (veramufenib) and Bristol-Myers Squibb (ipilimumab, the anti-melanoma agent discussed in ScienceWatch.com
last month) are collaborating on a two-agent approach. While stock exchanges quiver with excitement, let us not forget where the story really began and when—just nine years ago with a publication from the U.K.-based Cancer Genome Project funded by a medical research charity, the Wellcome Trust (H. Davies, et al., Nature, 41[6892]: 949-54, 2002).
A former deputy editor of The Lancet, David W. Sharp, M.A. (Cambridge), is a freelance writer living in Minchinhampton, Gloucestershire, U.K.
From
Journal of Viral HepatitisTwenty-four Weeks of Pegylated Interferon Plus Ribavirin Effectively Treat Patients With HCV Genotype 6a
Y. Q. Zhou; X. H. Wang; G. H. Hong; Y. Zhu; X. Q. Zhang; Y. J. Hu; Q. Mao
Authors and Disclosures
Posted: 09/05/2011; J Viral Hepat. 2011;18(8):595-600. © 2011 Blackwell Publishing
Introduction
Pegylated interferon (PEG-IFN) plus ribavirin is currently the standard treatment for patients with chronic hepatitis C virus (HCV) infection, and the optimal duration of treatment and expected response rate depend on the genotype of the infecting virus.
[1] HCV genotypes have been shown to have unique patterns of geographical distribution. HCV genotypes 1–3 are the predominant genotypes in Western Europe and the United States, and these genotypes have been the focus of most clinical trials to date. Forty-eight weeks of therapy are advised for patients with HCV genotype 1 (HCV-1) and 24 weeks for those with HCV-2/3.
[1,2] However, there is a general paucity of data on the treatment response in patients infected with other genotypes, including genotype 6.
[3–5]Hepatitis C virus genotype 6 (HCV-6) was traditionally believed to be confined to South-east Asia and was considered anecdotal elsewhere.
[3,6] However, recent studies demonstrated that the pockets of HCV-6 infections can be found worldwide.
[7–12] The optimal duration of treatment and expected response rate for patients with HCV-6 infection have not yet been determined.
[7,12–15] The few available results suggest that response to antiviral therapy in patients infected with HCV-6 is superior to that in patients infected with HCV-1 and may be similar to that in patients infected with HCV-2/3.
[7,12–15] Until now, there has been only one study that compared the treatment outcome of HCV-6 with that of HCV-2/3 directly.
[12] Moreover, previous reports have shown that the on-treatment virological response appears crucial for both tailoring the duration of therapy and influencing the treatment outcome,
[16,17] although no data are available concerning the association of the on-treatment virological response with the sustained virological response (SVR) in patients infected with HCV-6.
The frequencies of HCV-6a and HCV-3 have significantly increased in south-west China, and the traditional HCV-1b and HCV-2a are also present.[18] In recent years, patients with HCV-6a infection have been diagnosed and treated with PEG-IFN and ribavirin in the Southwest Hospital, in south-west China. The aims of this study were to determine the treatment outcome in patients with HCV-6a infection in comparison with HCV-2/3 as well as HCV-1b and assess the association of the on-treatment virological response with the SVR.
Full Text
Outbreak blamed on increased IV drug usage
MANITOWOC — Manitowoc County is seeing an increased number of Hepatitis C cases, but health officials say that's only one symptom of a bigger problem in the community.
"We have a large number of people who are addicted to IV drugs, and addiction is something that is very difficult to get treatment for," said Amy Wergin, public health nurse manager.
In 2010, Manitowoc County had 35 new cases of Hepatitis C, a slow-developing liver disease spread primarily by exposure to human blood from an infected person. So far this year, 44 cases have been reported with nearly 200 people still needing to be tested.
Liver Transplant
From
American Journal of TransplantationCyclosporine versus Tacrolimus Treated Liver Transplant Recipients With Chronic Hepatitis C
Outcomes Analysis of the UNOS/OPTN Database
W. D. Irish; S. Arcona; D. Bowers; J. F. Trotter
Authors and DisclosuresPosted: 09/05/2011; American Journal of Transplantation. 2011;11(8):1676-1675. © 2011 Blackwell Publishing
Introduction
Hepatitis C virus (HCV) is the leading cause of cirrhosis and hepatic failure leading to orthotopic liver transplantation (OLT) and accounts for approximately 40% of all liver transplants. Following transplantation, recurrence of HCV is nearly universal. Recurrent HCV is associated with significant complications and may lead to graft loss that requires retransplantation. The severity of recurrent HCV may be altered by the amount and type of immunosuppression. There is clear evidence that the treatment of acute cellular rejection (ACR) has a negative effect on recurrent HCV. Specifically, recurrent bolus therapy of corticosteroids and antibody therapy for ACR are perhaps the most important risk factors for severe recurrent HCV.
[1,2] However, there is no convincing data that any specific immunosuppressive agent is associated with worsening posttransplantation HCV. In particular, the role of calcineurin inhibitors (CNIs), in the acceleration of posttransplant viral replication of HCV and graft damage is unclear. Recent in vitro data suggests that cyclosporine (CSA-ME) may reduce the severity of recurrent HCV. Nakagawa et al. reported that cyclosporine may have an inhibitory effect on HCV replication in vitro.
[3] However, there is currently little clinical data to support these findings. In fact, a recent meta-analysis found no difference in severity of recurrent HCV for recipients receiving CSA-ME compared to TAC.
[4] Currently, there is a randomized trial underway which is specifically designed to assess the potential beneficial effect of cyclosporine on recurrent HCV. Because of the potential beneficial effects of cyclosporine on recurrent HCV, we undertook a study of the United Network for Organ Sharing (UNOS)/Organ Procurement and Transplantation Network (OPTN) database to retrospectively evaluate the long-term clinical outcomes and effects of maintenance immunosuppressive therapy, in particular, the CNIs CSA-ME versus TAC in a large contemporary cohort of patients who underwent OLT for HCV.
[5]Full Text;
AIDS
Dr David Cook, who is the Executive Vice President of IAVI, the International AIDS Vaccine Initiative, visited Sydney last week. He talks about the latest research into AIDS vaccines.
Stem Cells
They have already grown the bladder, urethra and windpipe which have been implanted into patients during clinical trials.
Now scientists have set their sights on replicating more complicated organs, including the heart, kidneys, liver, pancreas and thymus.
The advances could extend life expectancy and cut waiting times for transplants.
The developments were detailed at a conference on 'rejuvenation technologies' at Cambridge University, reported the Sunday Times.
Organiser Aubrey de Gray explained: 'We are seeing the emergence of a new era of medicine where the diseases of aging can be blocked or even reversed. These therapies are mostly in research now but eventually they will be commonplace.'
One of the speakers, Professor Paolo Macchiarini, of the Karolinska institute in Sweden, told how he impanted a laboratory-grown windpipe into a man sticken by throat cancer.
It had been created by using an artificial 'scaffold' designed in the shape of a windpipe which was impanted with the patient's stem cells.
'This could open new and very promising therapeutic possibilities for the thousands of patients who suffer from conditions that constrict the airway,' Mr Macchiarini said.
Professor Doris Taylor of Minnesota University, has already created a beating human heart by stripping dead cells from a donor organ and reseeding it with live ones.
And Professor Shay Soker of Wake Forest University in North Carolina, has created miniature human livers by seeding the protein skeleton from a rat's liver with human liver stem cells.
But there is one organ that can never be grown in a lab - the brain.
But scientists are trailing a drug called rilmenidine to help tackle Huntingtin's diseases which causes dementia and eventual death.
ScienceDaily (Sep. 4, 2011) — Human colon stem cells have been identified and grown in a petri dish in the lab for the first time. This achievement, made by researchers of the Colorectal Cancer Lab at the Institute for Research in Biomedicine (IRB Barcelona) and published in Nature Medicine, is a crucial advance towards regenerative medicine
Throughout life, stem cells of the colon regenerate the inner layer of our large intestine in a weekly basis. For decades scientists had evidences of the existence of these cells yet their identity remained elusive. Scientists led by the ICREA Professor and researcher at the Institute for Research in Biomedicine (IRB Barcelona) Eduard Batlle discovered the precise location of the stem cells in the human colon and worked out a method that allows their isolation and in vitro expansion, that is their propagation in lab-plates (petri dishes).
Growing cells outside the body generally requires providing the cells in a petri dish with the right mix of nutrients, growth factors and hormones. But in the same way that each of the more than 200 types of cells in our body differs from the others so too do optimal growing conditions for them in the lab. Consequently, human adult stem cell culture in labs has been practically impossible until now.
Batlle's team has also established the conditions for maintain living human colon stem cells (CoSCs) outside of the human body: "This is the first time that it has been possible to grow single CoSCs in lab-plates and to derive human intestinal stem cell lines in defined conditions in a lab setting," explains the IRB Barcelona researcher Peter Jung, first author of the study together with Toshiro Sato, from the University Medical Center Utrecht in The Netherlands.
The development, published by Batlle's research group in the journal Nature Medicine, arrives after more than 10 years of intense research focused on the characterization of the biology of the intestinal stem cells and its connection with cancer. The research has been made possible by close collaboration between Batlle's team and the group led by Hans Clevers at the Hubretcht Institute and University Medical Center Utrecht in The Netherlands, and María A. Blasco at the Spanish National Cancer Research Centre in Madrid (Spain).
"For years, scientists all over the world have been trying to grow intestinal tissue in lab-plates; testing different conditions; using different nutritive media. But because the vast majority of cells in this tissue are in a differentiated state in which they do not proliferate, they survived only for a few days," explains Jung. "The aim of this study was to find a way to identify and select individual CoSCs and to grow them while maintaining their undifferentiated and proliferative state in lab conditions. Thus, we would be able to model how they grow -- in number -- and differentiate into normal intestinal epithelial cells in lab-plates," continues Jung. The scientific community now has a defined 'recipe' for isolating CoSCs and deriving stable CoSCs lines, which have the capacity to grow undifferentiated for months. In fact, "now we can maintain stem cells in a plate up to 5 months or we can induce these cells to differentiate artificially, as they do inside our bodies."
"This achievement opens up an exciting new area of research with the potential to bring about a huge breakthrough in regenerative medicine," says Jung. Regenerative medicine -- or the idea of repairing the body by developing new tissues and organs as the old ones wear out -- involves growing new cells from patients into tissues and organs in a lab. However, the main element for making regenerative medicine a reality, namely adult stem cells, are just starting to be understood. "Now that guidelines for growing and maintaining colon stem cells in the lab are in place, we have an ideal platform that could help the scientific community to determine the molecular bases of gastrointestinal cell proliferation and differentiation. It is also suspected that alterations in the biology of CoSCs are at origin of several diseases affecting the gastrointestinal tract, such as colorectal cancer or Crohn's disease, an autoimmune and inflammatory disorder. Our discovery also paves the way to start exploring this exciting field," finishes Jung.
Research offers hope for better treatments for diabetes patients
JUPITER, FL, September 4, 2011 – In a joint study, scientists from The Scripps Research Institute and Harvard University's Dana-Farber Cancer Institute have established a new class of anti-diabetic compound that targets a unique molecular switch.
The finding paves the way for the development of anti-diabetic therapeutics with minimal adverse side effects plaguing currently available drugs such as Avandia (rosiglitazone), scheduled to be removed from pharmacy shelves this fall due to concerns about increased risk of heart attack.
The new study, led by Patrick R. Griffin, professor and chair of the Department of Molecular Therapeutics at Scripps Florida, Bruce Spiegelman, professor of cell biology at the Dana-Farber Cancer Institute, and Theodore Kamenecka, associate scientific director of medicinal chemistry at Scripps Florida, was published September 4, 2011, in the journal Nature. The study describes a new compound known as SR1664.
"In this study, we demonstrate that we have discovered novel compounds that work effectively through a unique mechanism of action on a well-validated clinical target for diabetes," said Griffin. "This unique mechanism of action appears to significantly limit side effects associated with marketed drugs. This study is a great example of interdisciplinary, inter-institutional collaboration with chemistry, biochemistry, structural biology, and pharmacology."
"It appears that we may have an opportunity to develop entire new classes of drugs for diabetes and perhaps other metabolic disorders," said Spiegelman.
Diabetes affects nearly 24 million children and adults in the United States, according to the America Diabetes Association.
A Viable Therapeutic Target
The study follows previous research by the authors published last year in Nature (Volume 466, Issue 7305, 451-456) that suggested an obesity-linked mechanism that may be involved in the development of insulin-resistance. In that research, the team found disruptions in various genes when a protein known as PPARγ undergoes phosphorylation (when a phosphate group is added to a protein) by the kinase Cdk5, an enzyme involved in a number of important sensory pathways.
The new study confirms that blockage of Cdk5's action on PPARG is a viable therapeutic approach for development of anti-diabetic agents. The new SR1664 compound is a potent binder to the nuclear receptor PPARG, but does not activate gene transcription via the receptor's normal mechanism.
While Griffin stressed the difficulty of fully assessing side effects of new compounds such as SR1664, the new research is extremely positive in that it clearly demonstrated fewer of the major well-documented side effects, such as weight gain or increased plasma volume, from SR1664 as compared to Avandia in diabetic mice.
While both the mice treated with Avandia and those treated with SR1664 demonstrated improved blood sugar levels, those treated with Avandia showed weight gain and increased fluid retention within a few days of beginning treatment; those being treated with SR1664 showed none of these side effects. In cell culture studies, SR1664 also appeared to have little effect on bone formation, nor did it increase fat generation in bone cells, another side effect of current therapies such as Avandia.
While S1664 likely will not be developed as a drug, it now serves as a molecular scaffolding for the creation of similar compounds with potential to treat diabetes. "With data in hand showing that our compounds are as efficacious as the currently marketed PPARG modulators, while demonstrating a significant improvement of side effects in limited studies, we are now advancing newer compounds with improved pharmaceutical properties into additional studies," Griffin said.
The first authors, denoted as equal contributors to this study, "Anti-Diabetic Actions of a Non-Agonist PPARG Ligand Blocking Cdk5-Mediated Phosphorylation," are Jang Hyun Choi and Alexander S. Banks of Dana-Farber Cancer Institute and Theodore M. Kamenecka and Scott A. Busby of The Scripps Research Institute. Other authors include Michael J. Chalmers, Naresh Kumar, Dana S. Kuruvilla, Youseung Shin, Yuanjun He, David Marciano, and Michael D. Cameron of Scripps Research; Dina Laznik of the Dana-Farber Cancer Institute; Michael J. Jurczak and Gerald I. Shulman of the Howard Hughes Medical Institute; Stephan C. Schürer and Dušica Vidović of the University of Miami; and John B. Bruning of Texas A&M University.
Pharmaceuticals
Prescription of very strong painkillers
listen now download audioA doctor from Adelaide complains about the prescription habits of doctors who prescribe morphine based medications for non-cancer pain.
Consumer Safety Marie McCullough and Gregory Thomas(The Philadelphia Inquirer, September 1, 2011)
"Eighteen months ago, the American Red Cross finished setting up new centers...to consolidate a crucial part of its blood business -- making sure donated blood is safe and recalling it if there is any doubt. By consolidating these duties...the Red Cross hoped to increase compliance with government safety rules, streamline operations, and reduce costs. But the Food and Drug Administration's [FDA] first -- and so far only -- inspection last fall found dysfunction and disorder at the new centers…The Red Cross says it has since addressed many of the problems at the new 'donor and client support centers'…The FDA declined to discuss the inspection report, the possibility of fines, or when it would reinspect the support centers. Inspections are done annually but are unannounced; the report was obtained through a Freedom of Information Act request...Since 1993, the Red Cross has been under a federal court order to improve the way it collects, processes, and tracks blood...Since [2003]...the FDA has fined the Red Cross $37 million for persistent lapses."
(CBS) Ever worry that someone in your doctor's office will accidentally expose you to HIV or another dangerous virus? That nightmare apparently came true for patients at one Midwestern clinic.
The Dean Clinic in Madison, Wis., informed state and local officials that 2,345 patients may have been exposed to hepatitis B, hepatitis C, and HIV between 2006 and 2011, when a diabetes educator working there used insulin demonstration pens and finger stick devices "inappropriately" during patient visits.......
 Bakers Union Marching Through the Labor Day Parade
Bakers Union Marching Through the Labor Day Parade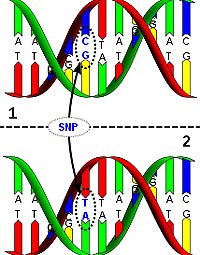
No comments:
Post a Comment