Related;Functional Dyspepsia; Chronic and persistent upper abdominal pain that's often related to eating
Definition of Liver pain
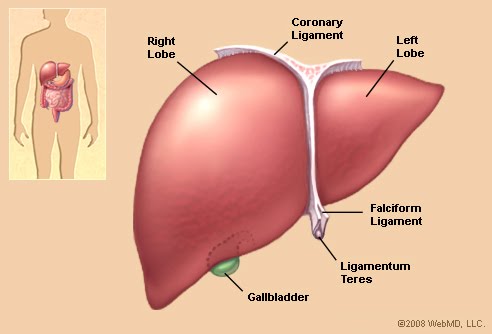
Pain coming from the liver. The liver does not contain nerve fibers that sense pain. Therefore, liver tissue can be cut, burned, or compressed without causing pain. There are pain fibers, however, in the liver's capsule, a thin layer of tissue that surrounds the liver tissue itself. The pain fibers of the capsule are stimulated when the capsule is stretched. Thus anything that stretches the capsule can cause liver pain. The common liver diseases that stretch the capsule are tumors that grow within the liver and inflammation of the liver that occurs, for example, with hepatitis of any cause. In the latter case, an accumulation of inflammatory cells and fluid within the liver is what stretches the capsule. The bile ducts that carry bile from the liver to the gallbladder and intestine as well as the gallbladder, also are surrounded by a thin layer of tissue that senses pain when it is stretched. Thus, stretching of the ducts due to problems within the ducts can lead to pain that may be difficult to distinguish from stretching of the capsule of the liver.
Answer: While the liver does indeed reside on the right side of the abdomen, with its bulk under the ribcage, pain in this area is not necessarily from the liver. There are several potential sources of pain in this part of the body. The gallbladder sits in a pocket surrounded by liver, and often can cause crampy intermittent pain when gallstones are present. The large intestine makes a sharp bend just under the liver in an area called the hepatic flexure. Gas can become trapped in this area and cause severe intermittent pain. If the liver becomes enlarged, the stretch of its capsure can cause a dull aching pain that is almost constant. Furthermore, the muscles of the rib cage can become torn or irritated and cause pain. A careful physical exam by an experienced physician can often separate these entities out.
Liver cysts occur in approximately 5% of the population. However, only about 5% of these patients ever develop symptoms. In general, cysts are thin-walled structures that contain fluid. Most cysts are single, although some patients may have several. The symptoms associated with liver cysts include upper abdominal fullness, discomfort, or pain. A small number of patients bleed into the cyst, which causes sudden and severe right upper quadrant and shoulder pain. The bleeding stops on its own, and the pain then improves over the next several days.. Continue reading...
Liver Pain During Pregnancy
Mar 22
Full story: Buzzle.com
Experiencing liver pain during pregnancy is a sign that there is something wrong with the liver.
Full story: Buzzle.com
Experiencing liver pain during pregnancy is a sign that there is something wrong with the liver.
There can be several reasons for experiencing liver pain during pregnancy. A pain in the liver may arise due to the strain of the growing womb on the nearby organs. However, persistent pain and discomfort in the abdominal region, especially in the upper right side may be a cause of concern, as it may be an indication of liver problems. It is essential to visit a gynecologist for a prompt diagnosis and treatment. Any changes in the body should be reported as soon as possible to the health care provider to avoid unwanted complications. Here we will discuss about the reasons for experiencing liver problems during pregnancy along with the methods of treatment.
Fatty liver refers to the infiltration of triglycerides and other fats into the liver cells, causing abnormal liver tests, inflammation and possibly permanent liver damage when left untreated. Because of improved imaging tests and frequent blood testing, fatty liver is now being diagnosed more frequently and non-alcoholic steatohepatitis (NASH), a form of fatty liver, has become the third most common liver disease in U.S. adults who are evaluated for increased liver enzymes.
While patients don't usually experience symptoms from fatty liver, it can be detected through an ultrasound or CT scan and by elevation in liver chemistries.
Occasionally, patients may experience a dull pain in the right upper abdomen or fatigue. To make an absolute diagnosis, a liver biopsy is performed.
While patients don't usually experience symptoms from fatty liver, it can be detected through an ultrasound or CT scan and by elevation in liver chemistries.
Occasionally, patients may experience a dull pain in the right upper abdomen or fatigue. To make an absolute diagnosis, a liver biopsy is performed.
.
Pain or discomfort usually refers to the pain in the upper right quadrant of the stomach. This pain also sometimes occurs in the right upper back and scapular area. The nature of the pain is usually a dull sensation combined with a subtle discomfort, which makes the patient actually become aware of the existence of the liver organ. This is a common symptom of chronic hepatitis, especially if there are problems in the gall bladder, such as gallstones or inflammation.
The liver parenchyma itself has no sensation, but the liver membrane, which forms a capsule covering the actual liver, is sensitive. When the liver becomes inflamed, conditions such as blood congestion, cell swelling (liver), increased secretion and retention of bile, and liver cell necrosis all increase the pressure to the liver membrane. This in turn causes the dull pain or discomfort in the liver area. During palpation, this area will also feel tender.
Pain or discomfort usually refers to the pain in the upper right quadrant of the stomach. This pain also sometimes occurs in the right upper back and scapular area. The nature of the pain is usually a dull sensation combined with a subtle discomfort, which makes the patient actually become aware of the existence of the liver organ. This is a common symptom of chronic hepatitis, especially if there are problems in the gall bladder, such as gallstones or inflammation.
The liver parenchyma itself has no sensation, but the liver membrane, which forms a capsule covering the actual liver, is sensitive. When the liver becomes inflamed, conditions such as blood congestion, cell swelling (liver), increased secretion and retention of bile, and liver cell necrosis all increase the pressure to the liver membrane. This in turn causes the dull pain or discomfort in the liver area. During palpation, this area will also feel tender.
The gallbladder is actually the more frequent the cause of this symptom since anatomically, gallbladder is literally “buried” in the lower surface of the liver. The gallbladder is sensitive to inflammation, pressure, and chemical stimulation, and can cause cramping, burning, and pricking pain. Since about 50% of chronic hepatitis patients have gallbladder problems, pain that originates in the gallbladder are often mistaken as liver pain. In order to find out whether the problem is in the gallbladder, an ultrasound examination may be necessary.
If inflammation or small gallstones (less than 2 cm in diameter) are causing the gall bladder pain, if the gallstones are large, then surgery may be needed to remove the stone(s) or the entire gall bladder.
If inflammation or small gallstones (less than 2 cm in diameter) are causing the gall bladder pain, if the gallstones are large, then surgery may be needed to remove the stone(s) or the entire gall bladder.
This pain is usually more obvious during acute episodes of chronic hepatitis.
Once the inflammation activities have been brought under controlled, the pain in the area should be reduced dramatically or be completely eliminated. However, sometimes sensations of pain will continue to exist even when the causes in the liver or gallbladder are controlled. Pain triggers in the brain may cause this phenomenon after a case of long-term chronic pain..
LiverPain and Risk factors
By Mayo Clinic staff
Each underlying problem that can lead to enlarged liver has a distinct set of risk factors.
For example: Alcohol abuse.
Men are more likely to abuse alcohol than women are. The risk of alcoholism is higher if you have a family history of the disease.
Depression and anxiety also increase the risk of alcohol abuse.
Nonalcoholic fatty liver disease.
Being overweight or obese is a major risk factor for nonalcoholic fatty liver disease. Having diabetes or abnormal cholesterol levels also increases the risk.
Hepatitis A.
You’re at increased risk of hepatitis A if you travel to or work in regions with high rates of hepatitis A. You’re also at risk if you’re a sexually active gay or bisexual man, you use illicit drugs, you work in a research setting where you may be exposed to the virus or you have hemophilia or receive clotting-factor concentrates for another medical condition.
Hepatitis B.
You’re at increased risk of hepatitis B if you have unprotected sex with more than one partner, you have a sexually transmitted disease, or you share needles during intravenous drug use. You’re also at risk if you live with someone who has a chronic hepatitis B infection, you have a job that exposes you to human blood or you received a blood transfusion or blood products before 1970.
Hepatitis C.
You’re at increased risk of hepatitis C if you inject or snort illicit drugs, you received an organ transplant before 1992, you’ve been exposed to infected blood or you received clotting factor concentrates before 1987. You’re also at risk if you have hemophilia and received blood products before 1992 or you’re receiving hemodialysis for kidney failure. Heart failure. Various factors increase the risk of heart failure, including high blood pressure, coronary artery disease, diabetes, kidney failure and congenital heart defects. Liver cancer. Chronic infection with hepatitis B or C is the most important risk factor for liver cancer. Cirrhosis — an irreversible scarring of the liver — diabetes, smoking and excessive alcohol consumption may increase risk as well.
Each underlying problem that can lead to enlarged liver has a distinct set of risk factors.
For example: Alcohol abuse.
Men are more likely to abuse alcohol than women are. The risk of alcoholism is higher if you have a family history of the disease.
Depression and anxiety also increase the risk of alcohol abuse.
Nonalcoholic fatty liver disease.
Being overweight or obese is a major risk factor for nonalcoholic fatty liver disease. Having diabetes or abnormal cholesterol levels also increases the risk.
Hepatitis A.
You’re at increased risk of hepatitis A if you travel to or work in regions with high rates of hepatitis A. You’re also at risk if you’re a sexually active gay or bisexual man, you use illicit drugs, you work in a research setting where you may be exposed to the virus or you have hemophilia or receive clotting-factor concentrates for another medical condition.
Hepatitis B.
You’re at increased risk of hepatitis B if you have unprotected sex with more than one partner, you have a sexually transmitted disease, or you share needles during intravenous drug use. You’re also at risk if you live with someone who has a chronic hepatitis B infection, you have a job that exposes you to human blood or you received a blood transfusion or blood products before 1970.
Hepatitis C.
You’re at increased risk of hepatitis C if you inject or snort illicit drugs, you received an organ transplant before 1992, you’ve been exposed to infected blood or you received clotting factor concentrates before 1987. You’re also at risk if you have hemophilia and received blood products before 1992 or you’re receiving hemodialysis for kidney failure. Heart failure. Various factors increase the risk of heart failure, including high blood pressure, coronary artery disease, diabetes, kidney failure and congenital heart defects. Liver cancer. Chronic infection with hepatitis B or C is the most important risk factor for liver cancer. Cirrhosis — an irreversible scarring of the liver — diabetes, smoking and excessive alcohol consumption may increase risk as well.
Description
Pain in the right upper quadrant (RUQ) can be caused by a wide variety of conditions. The age, sex and general condition of the patient will influence the likely diagnosis. History and examination will also focus the differential diagnosis. Features such as acute or chronic onset, weight loss, pyrexia, general malaise, and urinary or bowel symptoms may all help point to a diagnosis. It is important to decide if there is an acute abdomen.
Pain in the right upper quadrant (RUQ) can be caused by a wide variety of conditions. The age, sex and general condition of the patient will influence the likely diagnosis. History and examination will also focus the differential diagnosis. Features such as acute or chronic onset, weight loss, pyrexia, general malaise, and urinary or bowel symptoms may all help point to a diagnosis. It is important to decide if there is an acute abdomen.
Presentation
Symptoms
Enquire first about the pain:
Ask the patient to point to where it is. Does the patient use a single finger or is it more diffuse?
When did it start?
Was the onset sudden or gradual?
Is it continuous or intermittent?
Describe the nature of the pain - stabbing, burning, gripping, etc. Note the body language and use of hands.
Are there aggravating or relieving factors?
Is there any radiation?
Note past medical history.Make a systematic enquiry. The patient may volunteer information such as pyrexia, cough or dysuria.
Appetite
Any change in weight
Bowels
Urine
Smoking and drinking
Medication
Family history may be revealing.
Enquire first about the pain:
Ask the patient to point to where it is. Does the patient use a single finger or is it more diffuse?
When did it start?
Was the onset sudden or gradual?
Is it continuous or intermittent?
Describe the nature of the pain - stabbing, burning, gripping, etc. Note the body language and use of hands.
Are there aggravating or relieving factors?
Is there any radiation?
Note past medical history.Make a systematic enquiry. The patient may volunteer information such as pyrexia, cough or dysuria.
Appetite
Any change in weight
Bowels
Urine
Smoking and drinking
Medication
Family history may be revealing.
Signs
Note the general condition of the patient. Is the patient fairly well, shocked, pyrexial or dyspnoeic? Is there jaundice?
Note temperature, pulse rate and quality, and blood pressure.
The patient should be adequately disrobed and both the patient and the examiner should be in a comfortable position. A systematic examination of all the abdomen is required. Abdominal examination is described elsewhere.
Note the general condition of the patient. Is the patient fairly well, shocked, pyrexial or dyspnoeic? Is there jaundice?
Note temperature, pulse rate and quality, and blood pressure.
The patient should be adequately disrobed and both the patient and the examiner should be in a comfortable position. A systematic examination of all the abdomen is required. Abdominal examination is described elsewhere.
If the diagnosis is still elusive, examination of the respiratory system is indicated.
Differential diagnosis
Differential diagnosis
The crude differential diagnosis is vast but after adequate history and examination it should be very much smaller. The following order is not intended to indicate likelihood:
Liver and gallbladder disease
Liver disease is usually only painful if it stretches the capsule of the liver, as in congestive heart failure. The liver can be damaged by blunt trauma. Hepato-splenomegaly can occur with malignancy such as lymphoma or chronic myeloid leukaemia or with autoimmune disease including primary biliary cirrhosis.
Liver disease is usually only painful if it stretches the capsule of the liver, as in congestive heart failure. The liver can be damaged by blunt trauma. Hepato-splenomegaly can occur with malignancy such as lymphoma or chronic myeloid leukaemia or with autoimmune disease including primary biliary cirrhosis.
Gallstones are common and become more common as years advance. Most are asymptomatic but they can cause pain at any time.
Other gallbladder disease includes carcinoma of the gallbladder, which is always associated with stones too.
Ascending cholangitis has a classic triad of pain, fever and jaundice.
Bowel lesions
Lesions of the hepatic flexure include carcinoma, diverticulosis, ischaemic colitis, constipation and Crohn's disease.
Atypical acute appendicitis must be considered.
Recurrent symptoms can be caused by irritable bowel syndrome.
Meckel's diverticulum can present in a variety of ways, usually in children. The diagnosis is usually made at laparotomy. There is often blood loss per rectum.
Cardiovascular disease
Pain from a dissecting abdominal aortic aneurysm is usually most marked in the back and may originate in the chest and spread down the legs. Other arteries can have aneurysms and bleed.
Cardiac pain may occasionally present as upper abdominal pain.
Congestive cardiac failure may stretch the liver capsule.
Pain from a dissecting abdominal aortic aneurysm is usually most marked in the back and may originate in the chest and spread down the legs. Other arteries can have aneurysms and bleed.
Cardiac pain may occasionally present as upper abdominal pain.
Congestive cardiac failure may stretch the liver capsule.
Renal disorders
Pyelonephritis.
Nephrolithiasis.
Hydronephrosis.
Renal carcinoma.
Other disease of the kidney or ureter, including obstruction of the urinary tract.
Respiratory disease
Pain may arise from the right lower lobe of the lungs.
Lobar pneumonia
Infarction from pulmonary embolism. If this is suspected, check for evidence of deep vein thrombosis.
Endocrine or exocrine disease
Diabetic ketoacidosis.
Addisonian crisis.
Adrenal tuberculosis.
Metastatic carcinoma.
Pain from the pancreas tends to be central and higher in the back, often between the scapulae, although it can be atypical and misleading. Amylase is raised in intestinal obstruction but in acute pancreatitis it is very high.
Carcinoma of pancreas tends to produce an aching pain between the scapulae, eased on leaning forward.
Infections
Herpes zoster can present as pain before the typical vesicles appear on the skin. It is the skin that is tender rather than deeper.
Subphrenic abscess or even gas after laparotomy or, more often, laparoscopy. Pain may also be referred to the shoulder.
A rare condition is Fitz-Hugh and Curtis syndrome.2 There is inflammation of the liver capsule associated with genital tract infection. It is said to occur in up to one fourth of patients with pelvic inflammatory disease. Classically it presents as sharp, pleuritic RUQ pain but signs of salpingitis can be absent.
Pregnancy
The last trimester of pregnancy gives added problems.3 Minor elevations of liver enzymes may precede life-threatening disease, such as acute fatty liver of pregnancy (AFLP) or a syndrome of late pregnancy with Haemolysis, Elevated Liver enzyme levels, Low Platelet count (HELLP). Pre-eclampsia, HELLP syndrome, and AFLP form a spectrum of disease that ranges from mild symptoms to severe life-threatening multiorgan dysfunction. They have been shown to be the primary causes of severe hepatic dysfunction during pregnancy.
Other considerations
Pain may be referred from nerves in the spinal column or peripheral nerves that supply the area.
Recurrent abdominal pain is not uncommon in endurance athletes and its diagnosis can be difficult.4
Children are very non-specific about "tummy pain" and almost anything can present as such. Check ears, throat and urine. Mesenteric adenitis commonly presents with mild pyrexia and probably other lymphadenopathy.
Lesions associated with left upper quadrant pain may occasionally present on the other side. Situs inversus occurs in 1 person in 10,000.
This list is by no means exhaustive.
There are many other rarer causes of abdominal pain, including familial Mediterranean fever, tabes dorsalis and worm infestation. There is also the possibility of Münchhausen's syndrome.
Investigations
Investigations
The choice of investigations will depend upon the findings above.
FBC, ESR may give an indication of infection or an inflammatory process. Bleeding may cause anaemia. This may indicate malignancy.
Abnormal LFTs will occur if the liver is involved and in primary biliary cirrhosis there will be positive autoantibodies for mitochondria. It usually presents in a middle-aged woman with jaundice and pruritis.
Urinalysis may suggest urinary tract infection, including pyelonephritis or a lesion that causes slight bleeding, such as stones or malignancy.
Chest X-ray and lateral view may show a lesion of the right lower lobe. Collapse from infection and infarction look similar. Plain abdominal X-rays, erect and supine, may show abnormal bowel patterns, fluid levels or gas or fluid under the diaphragm. 70% of renal stones and 30% of gallstones are radio-opaque.
Colonoscopy or double contrast barium enema may be required for colonic lesions.
Ultrasound is useful to investigate the renal tract for stones or dilatation. It is the best way to detect gallstones5 and can also check the liver for enlargement and establish if it has an homogeneous pattern or areas of different echo density.
To investigate the spinal column, CT scan is good at revealing lesions of bone; however, MRI scan is better at showing lesions of the nervous system.
Abdominal CT or MRI scan may be useful to define a lesion. In overweight people, in whom ultrasound can be difficult, MRI scanning gives similar results.6 Radio-isotope imaging can show the liver and spleen.
Abstracts
Abstracts
published online 09 September 2010.
"Choledocholithiasis is the presence of a gallstone in the common bile duct. The stone may consist of bile pigments or calcium and cholesterol salts.Alternative NamesGallstone in the bile duct; Bile duct stone; Bile calculus; Biliary calculus"
Background & Aims:We assessed the temporal relationship between abdominal pain and elevation in liver function tests (LFTs) in patients with acute symptomatic choledocholithiasis..
Methods:Retrospective study of patients that presented within 12 hours of pain onset and were subsequently found to have choledocholithiasis.
Results:We identified 40 patients with complete medical records. Levels of aspartate and alanine aminotransferases (AST and ALT) correlated with duration of pain (Pearson correlation, r = 0.633 and 0.622 respectively, P < .001 for both); the correlation was not as strong for γ-glutamyl transpeptidase (GGT) (r = 0.326, P = .046) and was not significant for alkaline phosphatase or bilirubin. This temporal association was stronger in patients that had undergone cholecystectomy versus those with intact gallbladders (for ALT, r = 0.603 vs r = 0.311, respectively). Eighteen patients, evaluated within 6 hours of pain, had normal or minimal alterations in LFTs; transabdominal ultrasound was abnormal in 6 (sensitivity 33.3%). All had repeat LFTs within 24 hours (mean 10.3 ± 6.9 hours later) and large increases in ALT and aspartate aminotransferase levels (mean 10.5- and 6.8-fold respectively; P < .01 for both), intermediate increases in glutamyl transpeptidase levels, (mean 4-fold, P < .05), and no changes in alkaline phosphatase levels. This significant increase in LFTs was the only indication of biliary pathology before endoscopy in 11/18 patients. . Conclusions:Increasing duration of pain is associated with increasing LFTs (particularly transaminases) in patients with acute symptomatic choledocholithiasis. Patients with normal LFTs and ultrasound upon presentation should have repeat LFTs if biliary pain is suspected. The absence of significant biochemical abnormalities within the first 24 hours makes the diagnosis of symptomatic choledocholithiasis unlikely.
No comments:
Post a Comment