Silymarin use and liver disease progression in the Hepatitis C Antiviral Long-Term Treatment against Cirrhosis trial
.
Volume 33, Issue 1, pages 127–137, January 2011
N. D. Freedman1, T. M. Curto2, C. Morishima3, L. B. Seeff4, Z. D. Goodman5,
E. C. Wright6, R. Sinha1, J. E. Everhart7,
.
Article first published online: 2 NOV 2010
DOI: 10.1111/j.1365-2036.2010.04503.x
...
Background Silymarin is the most commonly used herbal product for chronic liver disease; yet, whether silymarin protects against liver disease progression remains unclear.
.
Aim
.
Methods
.
Results
.
Finally, we analysed changes in morphometric collagen content across study biopsies using repeated analysis of variance, assuming an autoregressive covariance structure with the PROC MIXED function of sas 9.1. Again, analyses were restricted to patients who had not had an outcome prior to a particular scheduled study biopsy. Time (baseline, biopsy one, and biopsy two) and silymarin use (former and current) were included in the model as fixed effects. Adjustment for age and gender did not alter risk estimates and so were not included in the final models. Possible differences between the collagen content of biopsies taken from former or current silymarin users were compared with the collagen content of biopsies taken from never silymarin users by the Mann–Whitney test.
.
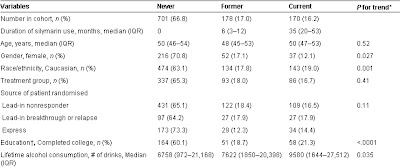
At baseline, 17% (178/1049) of patients were former users of silymarin and 16% (170/1049) of patients were current users compared to 67% (701/1049) who reported never using silymarin (Table 1).

.
IQR: interquartile range; AST, aspartate aminotransferase; ALT, alanine aminotransferase; Alk. Phos., alkaline phosphatase; HCV, hepatitis C virus.
* Mantel-Haenszel test for trend for categorical variables. Jonckheere-Terpstra test for trend for continuous variables.
† Data not available for all participants: coffee was available for 791 participants; collagen content for 558 patients; education available for 1045 participants; oesophageal varices for 1016 participants; SF-36 scores for 1043 participants.
At baseline, 621 patients had fibrosis and 428 patients had cirrhosis. During 4758 person-years of follow-up (median: 5.5 years per patient, interquartile range: 3.0–6.6 years), 384 patients had a two point increase in fibrosis score (TPI) from baseline or had a clinical outcome for liver disease.
Combining these endpoints, we observed an inverse association between baseline silymarin use and liver disease progression
(Table 2).
In crude models, the relative risk (RR) associated with former use of silymarin was 0.87 (95% CI: 0.66–1.15), whereas the RR for current use was 0.73 (95% CI: 0.54–0.98; P-trend across categories = 0.029). Upon stratification by outcome, current silymarin use was associated with less TPI (RR for current vs. never use of silymarin, 0.54, 95% CI: 0.32–0.93; P-trend = 0.015), but had no association with clinical outcomes (RR for current vs. never, 0.86, 0.61–1.20; P-trend = 0.42). Multivariate adjustment for age, education, race/ethnicity, gender, lifetime alcohol use, diabetes, coffee intake, ever use of other herbal products besides silymarin, mental and physical quality of life scores, baseline cirrhosis, AST/ALT ratio, albumin, platelets, bilirubin and oesophageal varices only modestly affected risk estimates. After multivariate adjustment, the RR for current vs. never use of silymarin was 0.57 (95% CI: 0.33–1.00; P-trend = 0.042) for TPI and 1.09 (95% CI: 0.77–1.56; P-trend = 0.89) for clinical outcomes.
.
Association of silymarin use with liver disease progression in 1049 participants of the HALT-C trial
Click To Enlarge (Table 2).
.

TPI, two point increase in Ishak fibrosis score; RR, relative risk; CI, confidence interval.
* Excluding 56 participants with fibrosis at baseline who did not receive follow-up biopsies or have a clinical outcome.
† Adjusted for continuous age, lifetime alcohol use and coffee intake along with categorical variables for education (high school or less, some post high school, completed college), race/ethnicity (Caucasian, African American, Hispanic and other), gender, diabetes and ever use of other herbal products besides silymarin, such as green tea, garlic, ginseng and Echinacea.
‡ Additionally adjusted for continuous mental and physical SF-36 quality of life scores, AST/ALT ratio, albumin, platelets, bilirubin, as well as categorical variables for cirrhosis status at baseline and presence or absence of oesophageal varices
.
Duration of silymarin use, prior to baseline, was also assessed. Compared to never users, patients who used silymarin for up to the median duration (16.6 months) had an RR for TPI of 0.93 (0.58–1.51), whereas patients who used silymarin for greater than the median duration had an RR of 0.51 (95% CI: 0.30–0.90; P-trend = 0.026). The RRs for clinical outcomes for the same two categories of silymarin use were 0.86 (95% CI: 0.61–1.21) and 0.94 (95% CI: 0.66–1.35; P-trend = 0.57) respectively (data not shown in table).
In addition to silymarin use at baseline, we examined silymarin use over the course of the study. At the time of the second biopsy, three and a half years after randomisation, 69% of baseline users continued to use silymarin (88/128), whereas only 3% of baseline non-users (15/477) had started use. The risk of TPI among patients with fibrosis who continued to use silymarin throughout the study was 0.55 (95% CI: 0.29–1.03; 68 patients, 11 events), whereas the risk of TPI among patients who stopped using silymarin during follow-up was 0.66 (95% CI: 0.23–1.87; 20 patients, 4 events) (data not shown in table).
Silymarin was the most commonly used herbal product in the HALT-C trial. Fourteen percent of patients used an herbal product other than silymarin (n = 142). Use of a nonsilymarin herbal product had no association with either TPI (0.92, 95% CI: 0.57–1.48) or clinical outcomes (0.87, 95% CI: 0.60–1.25) (data not shown in table).
Among those with fibrosis, comparing current users of silymarin with never users, the RR for TPI was 0.19 (95% CI: 0.02–2.05; 16 events) for patients with an Ishak score of 2 at baseline, 0.48 (95% CI: 0.22–1.04; 87 events) for patients with an Ishak score of 3 at baseline, and 1.04 (95% CI: 0.37–2.90; 49 events) for patients with an Ishak score of 4 at baseline (data not shown in table). For those with fibrosis at baseline, we also examined the distribution of Ishak scores at year 1.5 and year 3.5 protocol biopsies. The distribution of Ishak scores was similar between former and never silymarin users for both biopsies (P more then 0.30). For current silymarin users vs. never silymarin users, P-values for differences in the distribution of Ishak scores were 0.097 and 0.0059, for year 1.5 and year 3.5 biopsies respectively
Click Here To View (Figure 1).
Figure 1.
Distribution at each biopsy for 621 patients without cirrhosis at baseline (Ishak score of 2, 3, or 4).
Repeat protocol biopsies were performed 1.5 years (Biopsy 1, 524 patients) and 3.5 years after randomisation (Biopsy 2, 443 patients). The P-values for the distribution of Ishak scores of former vs. never silymarin users were 0.086, 0.30 and 0.47 for baseline, biopsy 1 and biopsy 2 respectively. For current silymarin users vs. never silymarin users, P-values for the distribution of Ishak scores at each biopsy were 0.42, 0.097 and 0.0059 respectively.
No association for clinical outcomes was found for those with either fibrosis or cirrhosis at baseline (RR for current use vs. never use, 1.36, 95% CI: 0.74–2.50, P-trend = 0.32, 98 events and 0.97, 95% CI: 0.61–1.53, P-trend = 0.41, 176 events, for fibrosis and cirrhosis respectively). The association between silymarin and clinical outcomes was also similar for outcomes occurring during years zero through four (RR for current vs. never use, 1.20, 95% CI: 0.78–1.86; P-trend = 0.85, 173 events) and five through eight of follow-up (0.88, 95% CI: 0.47–1.63; P-trend = 0.88, 101 events) (data not shown in table). Kaplan–Meier curves for clinical outcomes among current, former and never users of silymarin were similar
P = 0.657). In a secondary analysis of 88 incident cases of HCC, compared to never use, the RR for former and current users was 1.15 (95% CI: 0.62–2.13) and 1.60 (95% CI: 0.93–2.76) respectively. This possible effect was restricted to events occurring during the first 4 years (HR: 1.96, 95% CI: 0.95–4.05; 47 events), but not years five-eight of follow-up (HR: 1.26, 95% CI: 0.54–2.94; 41 events).
.
Click Here To View : Figure 2;
Kaplan–Meier survival analysis of time to first clinical outcome by stratum of baseline silymarin use (never, former, and current; P = 0.657) .
Finally, we examined the association between silymarin use and biopsy collagen content as measured by morphometric image analysis (Table 3).
The collagen content of each study biopsy appeared generally similar in former and never users of silymarin. But, the study biopsies of baseline silymarin users tended to have a lower collagen content than study biopsies of never users. For example, the mean collagen content on the year 3.5 biopsy was 0.071 (standard deviation = 0.069) among current silymarin users and 0.090 (standard deviation = 0.085) among never users, P-value = 0.061. The overall P-value comparing the change in collagen content across repeated biopsies in baseline silymarin users relative to never users was 0.037. After stratification by baseline cirrhosis status, the association between silymarin use with change in collagen content across repeated study biopsies persisted in both patients with fibrosis (overall P-value = 0.034) and those with cirrhosis (overall P-value = 0.011) at baseline.
.
Click Here To Enlarge (Table 3).

Assessment of morphometric collagen content was limited to biopsies with at least 10 mm2 of tissue, including 558 biopsies at baseline, 550 biopsies at year 1.5, and 409 biopsies at year 3.5.
* Mann–Whitney test for the difference between mean collagen content in former or current silymarin users relative to never users.
† P-value for the overall effect of silymarin use on morphometric collagen content across repeated biopsies was assessed by repeated-measures analysis of variance assuming an autoregressive covariance structure. Time (baseline, biopsy 1, and biopsy 2) and silymarin use were included in the models as fixed effects .
.
Discussion
/
In a large prospective cohort of individuals with advanced hepatitis C- related chronic liver disease, no clinical benefit was found for current silymarin use at baseline. In addition, we observed a nonsignificant increase in HCC risk among current silymarin users, which was present only in the first 4 years of follow-up. Baseline silymarin use was associated with less liver disease progression as measured by a two-point increase in Ishak fibrosis score as well as in the distribution of fibrosis scores in follow-up biopsies. A dose–response with duration of use was observed. Current use of silymarin at baseline, but not former use prior to baseline, was associated inversely with biopsy collagen content, regardless of whether patients had fibrosis or cirrhosis.
.
Silymarin has been used to treat liver disease for thousands of years.6, 27
Furthermore, results from animal, in vitro and clinical studies suggest that silymarin has possible anti-inflammatory,9–11 anti-viral,11–14 antioxidant10, 15 and antifibrotic effects.10, 16, 17 Yet, few clinical and observational studies have evaluated the effect of silymarin on liver disease progression and clinical outcomes in humans. Previous studies had small size, limited power to detect associations, and yielded mixed results.6, 27 For example, one trial of 170 patients with alcohol-related liver disease showed an effect of silymarin on survival,28 whereas a second trial of 200 patients showed similar survival rates in the randomised and control arms.29 Even fewer data are available for hepatitis C-related liver disease. Data from an Egyptian randomised trial of 141 patients showed no effect for silymarin on outcomes.30, 31
.
It is not clear why silymarin was associated with a reduction in rate of fibrosis progression, but not with clinical outcomes in our study. One possibility is that in order to exert an effect, silymarin must be used early in the disease progression process. In support of this hypothesis, silymarin seemed to have an effect on histological progression if patients had an Ishak score of 2 or 3 at baseline, but no effect on individuals with a score of 4 at baseline. On the other hand, silymarin had no effect on clinical outcomes for individuals with either cirrhosis or fibrosis at baseline, or for outcomes occurring during the first 4 years, or years five-eight of follow-up. It remains possible, however, that follow-up was too short to see an effect on clinical outcomes.
Fibrosis progression is not the sole determinant of subsequent decompensation or complications of portal hypertension. As such, it is also possible that silymarin does not have a beneficial effect on other determinants of clinical outcomes.32 Alternatively, differences between histological progression and clinical outcomes could simply reflect chance.
.
Strengths of our study include assessment of silymarin use before disease progression, the large number of patients with advanced hepatitis C-related liver disease, comprehensive assessment of clinical, demographic and lifestyle information, and careful assessment of clinical and histological outcomes. The major limitation was a complete lack of information on the amount of silymarin patients used per day. We also lacked information on how silymarin was prepared.
.
Patients in the HALT-C trial probably used many different dosages and formulations of silymarin and even for individual patients, preparations probably varied day by day and week by week. Furthermore, it is unlikely that patients would have ingested pharmacological doses of silymarin as have shown effect in vitro, clinical, and animal studies. For example, a recent study of 36 patients observed an effect of intravenously (i.v.) administered silymarin (as silibinin) on hepatitis C viral level,14 although a study with similar dosing of orally administered silymarin showed no effect.33 Most likely, patients in HALT-C used less silymarin than those in the i.v. study. Further complicating interpretation is that the pharmacokinetics of silymarin may be altered by fibrosis. A recent study administered a standard silymarin dose to cirrhotics and healthy volunteers. In response to silymarin treatment, serum flavonolignans were higher in the cirrhotic volunteers.34 Finally, not all study biopsies were large enough to have morphometric analysis performed, a potential source of selection bias. Indeed, patients with cirrhosis were less likely to receive all biopsies.21 Yet, as we observed an apparent inverse association between silymarin use and collagen content, such a bias, if anything, would probably attenuate the observed association between silymarin use and collagen content.
.
In the HALT-C trial, use of silymarin was associated with Caucasian race, completing college and a higher SF-36 physical quality of life score, suggesting that silymarin use might be a marker for a large number of other lifestyle factors. We adjusted our risk estimates for these and other possible confounders. After adjustment, risk estimates were only modestly altered. In addition, the observed effect of silymarin does not simply reflect a propensity to use herbal products.
Using herbal products, other than silymarin, had no association with either histological progression or clinical outcomes in our study. Nevertheless, as an observational study, the inverse association observed between silymarin use and histological progression could reflect another exposure or chance. We did not have any information on brand or dosage of silymarin.
However, this limitation is reflective of the difficulty in detailing patient behaviour outside controlled studies. Many, if not most, patients with currently incurable liver disease seek alternative, unapproved therapies that cannot be easily quantified, yet deserve evaluation.
In summary, among individuals with advanced hepatitis-C-associated liver disease, we observed an inverse association between silymarin use and the progression of liver disease from fibrosis to cirrhosis, but no evidence for an effect on clinical outcomes. As our results are from an observational study, it is possible that the observed beneficial effect on liver disease progression is due to chance. Future studies with a comprehensive assessment of silymarin dose are needed to replicate these findings. Nevertheless, our results provide support for conducting additional studies of silymarin, including intervention trials with defined dosage regimens and standard silymarin product. Such studies would be most appropriate for patients who have not responded to or are not candidates for anti-viral therapy and have limited other treatment options. Importantly, our results do not support the use of ad hoc dosing of silymarin by patients with chronic liver disease..
. /
Declaration of personal interests: None. In addition to the authors of this manuscript, the following individuals were instrumental in the planning, conduct and/or care of patients enrolled in this study at each of the participating institutions as follows:
University of Massachusetts Medical Center, Worcester, MA: (Contract N01-DK-9-2326) Gyongyi Szabo, MD, Barbara F. Banner, MD, Maureen Cormier, RN, Donna Giansiracusa, RN.
University of Connecticut Health Center, Farmington, CT: (Grant M01RR-06192) Herbert L. Bonkovsky, MD, Gloria Borders, RN, Michelle Kelley, RN, ANP.
Saint Louis University School of Medicine, St Louis, MO: (Contract N01-DK-9-2324) Adrian M. Di Bisceglie, MD, Bruce Bacon, MD, Brent Neuschwander-Tetri, MD, Elizabeth M. Brunt, MD, Debra King, RN.
Massachusetts General Hospital, Boston, MA: (Contract N01-DK-9-2319, Grant M01RR-01066; Grant 1 UL1 RR025758-01, Harvard Clinical and Translational Science Center) Jules L. Dienstag, MD, Raymond T. Chung, MD, Andrea E. Reid, MD, Atul K. Bhan, MD, Wallis A. Molchen, David P. Lundmark.
University of Colorado Denver, School of Medicine, Aurora, CO: (Contract N01-DK-9-2327, Grant M01RR-00051, Grant 1 UL1 RR 025780-01), Gregory T. Everson, MD, Thomas Trouillot, MD, Marcelo Kugelmas, MD, S. Russell Nash, MD, Jennifer DeSanto, RN, Carol McKinley, RN.
University of California - Irvine, Irvine, CA: (Contract N01-DK-9-2320, Grant M01RR-00827) Timothy R. Morgan, MD, John C. Hoefs, MD, John R. Craig, MD, M. Mazen Jamal, MD, MPH, Muhammad Sheikh, MD, Choon Park, RN.
University of Texas Southwestern Medical Center, Dallas, TX: (Contract N01-DK-9-2321, Grant M01RR-00633, Grant 1 UL1 RR024982-01, North and Central Texas Clinical and Translational Science Initiative) William M. Lee, MD, Thomas E. Rogers, MD, Peter F. Malet, MD, Janel Shelton, Nicole Crowder, LVN, Rivka Elbein, RN, BSN, Nancy Liston, MPH.
University of Southern California, Los Angeles, CA: (Contract N01-DK-9-2325, Grant M01RR-00043) Karen L. Lindsay, MD, MMM, Sugantha Govindarajan, MD, Carol B. Jones, RN, Susan L. Milstein, RN.
University of Michigan Medical Center, Ann Arbor, MI: (Contract N01-DK-9-2323, Grant M01RR-00042, Grant 1 UL1 RR024986, Michigan Center for Clinical and Health Research) Anna S. Lok, MD, Robert J. Fontana, MD, Joel K. Greenson, MD, Pamela A. Richtmyer, LPN, CCRC, R. Tess Bonham, BS.
Virginia Commonwealth University Health System, Richmond, VA: (Contract N01-DK-9-2322, Grant M01RR-00065) Mitchell L. Shiffman, MD, Richard K. Sterling, MD, MSc, Melissa J. Contos, MD, A. Scott Mills, MD, Charlotte Hofmann, RN, Paula Smith, RN.
Liver Diseases Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD: Marc G. Ghany, MD, T. Jake Liang, MD, David Kleiner, MD, PhD, Yoon Park, RN, Elenita Rivera, RN, Vanessa Haynes-Williams, RN.
National Institute of Diabetes and Digestive and Kidney Diseases, Division of Digestive Diseases and Nutrition, Bethesda, MD: Patricia R. Robuck, PhD, Jay H. Hoofnagle, MD.
University of Washington, Seattle, WA: (Contract N01-DK-9-2318) David R. Gretch, MD, PhD, Minjun Chung Apodaca, BS, ASCP, Rohit Shankar, BC, ASCP, Natalia Antonov, M. Ed.
New England Research Institutes, Watertown, MA: (Contract N01-DK-9-2328) Kristin K. Snow, MSc, ScD, Anne M. Stoddard, ScD, Margaret C. Bell, MS, MPH.
Armed Forces Institute of Pathology, Washington, DC: Fanny Monge, Michelle Parks.
Data and Safety Monitoring Board Members: (Chair) Gary L. Davis, MD, Guadalupe Garcia-Tsao, MD, Michael Kutner, PhD, Stanley M. Lemon, MD, Robert P. Perrillo, MD.
Declaration of funding interests: This study was funded in part by the National Institute of Diabetes & Digestive & Kidney Diseases (contract numbers are listed below). Additional support was provided by the National Institute of Allergy and Infectious Diseases (NIAID), the National Cancer Institute, the National Center for Minority Health and Health Disparities and by General Clinical Research Center and Clinical and Translational Science Center grants from the National Center for Research Resources, National Institutes of Health (grant numbers are listed in the Acknowledgement). This research was also supported in part by the Intramural Research Program of the National Cancer Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health. Additional funding to conduct this study was supplied by Hoffmann-La Roche, Inc., through a Cooperative Research and Development Agreement (CRADA) with the National Institutes of Health.
Jump to…Top of pageAbstractIntroductionPatients and methodsResultsDiscussionAcknowledgementsReferences
.
References
Abstract
Introduction
Patients and methods
Results
Discussion
Acknowledgements
References
1
Lavanchy D. The global burden of hepatitis C. Liver Int 2009; 29(Suppl. 1): 74–81.
Direct Link:
Abstract
Full Article (HTML)
PDF(178K)
References
2
Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002; 347: 975–82.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 2484
3
Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet 2001; 358: 958–65.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 2772
4
Stickel F, Schuppan D. Herbal medicine in the treatment of liver diseases. Dig Liver Dis 2007; 39: 293–304.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 32
5
Verma S, Thuluvath PJ. Complementary and alternative medicine in hepatology: review of the evidence of efficacy. Clin Gastroenterol Hepatol 2007; 5: 408–16.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 9
6
Rambaldi A, Jacobs BP, Iaquinto G, Gluud C. Milk thistle for alcoholic and/or hepatitis B or C liver diseases – a systematic cochrane hepato-biliary group review with meta-analyses of randomized clinical trials. Am J Gastroenterol 2005; 100: 2583–91.
Direct Link:
7
Seeff LB, Curto TM, Szabo G, et al. Herbal product use by persons enrolled in the Hepatitis C Antiviral Long-Term Treatment against Cirrhosis (HALT-C) trial. Hepatology 2008; 47: 605–12.
Direct Link:
Abstract
Full Article (HTML)
PDF(239K)
References
8
Shibano M, Lin AS, Itokawa H, Lee KH. Separation and characterization of active flavonolignans of Silybum marianum by liquid chromatography connected with hybrid ion-trap and time-of-flight mass spectrometry (LC-MS/IT-TOF). J Nat Prod 2007; 70: 1424–8.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 7
9
Morishima C, Shuhart MC, Wang CC, et al. Silymarin inhibits in vitro T-cell proliferation and cytokine production in hepatitis C virus infection. Gastroenterology 2010; 138: 671–81.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 5
10
Trappoliere M, Caligiuri A, Schmid M, et al. Silybin, a component of sylimarin, exerts anti-inflammatory and anti-fibrogenic effects on human hepatic stellate cells. J Hepatol 2009; 50: 1102–11.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 3
11
Polyak SJ, Morishima C, Shuhart MC, et al. Inhibition of T-cell inflammatory cytokines, hepatocyte NF-kappaB signaling, and HCV infection by standardized Silymarin. Gastroenterology 2007; 132: 1925–36.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 31
12
Ahmed-Belkacem A, Ahnou N, Barbotte L, et al. Silibinin and related compounds are direct inhibitors of hepatitis C virus RNA-dependent RNA polymerase. Gastroenterology 2010; 138: 1112–22.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 1
13
Bonifaz V, Shan Y, Lambrecht RW, et al. Effects of silymarin on hepatitis C virus and haem oxygenase-1 gene expression in human hepatoma cells. Liver Int 2009; 29: 366–73.
Direct Link:
Abstract
Full Article (HTML)
PDF(333K)
References
14
Ferenci P, Scherzer TM, Kerschner H, et al. Silibinin is a potent antiviral agent in patients with chronic hepatitis C not responding to pegylated interferon/ribavirin therapy. Gastroenterology 2008; 135: 1561–7.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 24
15
Pietrangelo A, Borella F, Casalgrandi G, et al. Antioxidant activity of silybin in vivo during long-term iron overload in rats. Gastroenterology 1995; 109: 1941–9.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 87
16
Boigk G, Stroedter L, Herbst H, et al. Silymarin retards collagen accumulation in early and advanced biliary fibrosis secondary to complete bile duct obliteration in rats. Hepatology 1997; 26: 643–9.
Direct Link:
Abstract
PDF(705K)
References
17
Dehmlow C, Erhard J, De Groot H. Inhibition of Kupffer cell functions as an explanation for the hepatoprotective properties of silibinin. Hepatology 1996; 23: 749–54.
Direct Link:
Abstract
PDF(218K)
References
18
Di Bisceglie AM, Shiffman ML, Everson GT, et al. Prolonged therapy of advanced chronic hepatitis C with low-dose peginterferon. N Engl J Med 2008; 359: 2429–41.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 85
19
Ishak K, Baptista A, Bianchi L, et al. Histological grading and staging of chronic hepatitis. J Hepatol 1995; 22: 696–9.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 1643
20
Goodman ZD, Becker RL Jr, Pockros PJ, Afdhal NH. Progression of fibrosis in advanced chronic hepatitis C: evaluation by morphometric image analysis. Hepatology 2007; 45: 886–94.
Direct Link:
Abstract
Full Article (HTML)
PDF(467K)
References
21
Goodman ZD, Stoddard AM, Bonkovsky HL, et al. Fibrosis progression in chronic hepatitis C: morphometric image analysis in the HALT-C trial. Hepatology 2009; 50: 1738–49.
Direct Link:
Abstract
Full Article (HTML)
PDF(1037K)
References
22
Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973; 60: 646–9.
Direct Link:
Abstract
PDF(430K)
References
23
Lok AS, Seeff LB, Morgan TR, et al. Incidence of hepatocellular carcinoma and associated risk factors in hepatitis C-related advanced liver disease. Gastroenterology 2009; 136: 138–48.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 33
24
Cox DR. Regression models and life-tables. J R Stat Soc Series B Stat Methodol 1972; 34: 187.
25
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–83.
CrossRef,
PubMed,
Web of Science®
26
Ghany MG, Lok AS, Everhart JE, et al. Predicting clinical and histologic outcomes based on standard laboratory tests in advanced chronic hepatitis C. Gastroenterology 2010; 138: 136–46.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 5
27
Mayer KE, Myers RP, Lee SS. Silymarin treatment of viral hepatitis: a systematic review. J Viral Hepat 2005; 12: 559–67.
Direct Link:
Abstract
Full Article (HTML)
PDF(90K)
References
28
Ferenci P, Dragosics B, Dittrich H, et al. Randomized controlled trial of silymarin treatment in patients with cirrhosis of the liver. J Hepatol 1989; 9: 105–13.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 216
29
Pares A, Planas R, Torres M, et al. Effects of silymarin in alcoholic patients with cirrhosis of the liver: results of a controlled, double-blind, randomized and multicenter trial. J Hepatol 1998; 28: 615–21.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 128
30
Strickland GT, Tanamly MD, Tadros F, et al. Two-year results of a randomised double-blinded trial evaluating silymarin for chronic hepatitis C. Dig Liver Dis 2005; 37: 542–3.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 12
31
Tanamly MD, Tadros F, Labeeb S, et al. Randomised double-blinded trial evaluating silymarin for chronic hepatitis C in an Egyptian village: study description and 12-month results. Dig Liver Dis 2004; 36: 752–9.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 17
32
Cho YK, Yun JW, Park JH, et al. Deleterious effects of silymarin on the expression of genes controlling endothelial nitric oxide synthase activity in carbon tetrachloride-treated rat livers. Life Sci 2009; 85: 281–90.
CrossRef,
PubMed,
ChemPort,
Web of Science®
33
Gordon A, Hobbs DA, Bowden DS, et al. Effects of Silybum marianum on serum hepatitis C virus RNA, alanine aminotransferase levels and well-being in patients with chronic hepatitis C. J Gastroenterol Hepatol 2006; 21: 275–80.
Direct Link:
Abstract
Full Article (HTML)
PDF(136K)
References
34
Schrieber SJ, Wen Z, Vourvahis M, et al. The pharmacokinetics of silymarin is altered in patients with hepatitis C virus and nonalcoholic fatty liver disease and correlates with plasma caspase-3/7 activity. Drug Metab Dispos 2008; 36: 1909–16.
CrossRef,
PubMed,
ChemPort,
Web of Science® Times Cited: 8
No comments:
Post a Comment