 Interferons are a group of naturally occurring proteins and glycoproteins which have antiviral, antineoplastic, and immune-regulation properties.
Interferons are a group of naturally occurring proteins and glycoproteins which have antiviral, antineoplastic, and immune-regulation properties. Interferon may cause retinal complications as well--and more often than other systemic medication (e.g., hydroxychloroquine or phenothiazines). It may cause vision loss. Some reports state up to 57% of patients taking interferon experience retinopathy (first reported in US in 1993).
----------------------
Rarer eye findings
Impaired vision
Retinal artery/vein occlusions
Bilateral oculomotor nerve paralysis
Mydriasis
Anterior ischemic optic neuropathy
Microaneurysms
Subconjunctival hemorrhages
Vascular tortuosity and congestion
Early onset of cataracts
Vitreous hemorrhage
CME
Photophobia
Ocular side effects are more likely if patient . . .
Also has diabetes mellitus, hypertension, or anemia
Is older, female, or has arterial sclerosis
Is on higher dose of interferon
Is also taking antidepressant medication paroxetine (a serotonin-reuptake inhibitor)
Why is this damage occurring?
So, what should be our standard of care?
At baseline, a full fundoscopic exam with photos is helpful to monitor the patient both pre- and post-treatment.
Patient should receive baseline fundus exam before starting interferon treatment.
Patient should be followed every 3 months.
Take fundus photos to monitor for progression.
Give patient Amsler grid for home monitoring.
Instruct patient to return ASAP if notes any changes in vision.
If sight is threatened, contact patient's MD to weigh the risks/benefits of discontinuing the medication.
At baseline, a full fundoscopic exam with photos is helpful to monitor the patient both pre- and post-treatment.
Retinopathy associated with pegylated interferon and ribavirin treatment for chronic hepatitis C
.
Retinopathy is associated with the use of interferon and ribavirin for the treatment of chronic hepatitis C. Common ocular complications include cotton wool spots, retinal hemorrhages, and macular edema.
.
A 53-year-old black man with a history of drug and alcohol abuse was admitted to the Department of Veterans Affairs clinic for substance abuse treatment. Results of a liver biopsy showed chronic hepatitis C, and treatment with interferon and ribavirin was initiated. A comprehensive eye examination was performed just before the initiation of treatment, and the patient was then periodically monitored for the presence of retinopathy.
Conclusions
Although this patient was visually asymptomatic, and his retinopathy resolved during treatment, we chose to monitor the patient monthly during treatment because of the risk of serious (although rare) ocular complications.
Indian J Ophthalmol.
doi: 10.4103/0301-4738.60088.
PMCID: PMC2854447
Copyright © Indian Journal of Ophthalmology
Cystoid macular edema and visual loss as sequelae to interferon alpha treatment of systemic hepatitis C
Hepatitis C virus infection and interferon treatment may be associated with retinopathy but visual function is generally unaffected. This paper reports the rare occurrence of unilateral macular edema with visual loss. We present an interventional case report with fundus photograph and optical coherence tomography (OCT).
This report shows that cystoid macular edema may rarely occur in association with hepatitis C infection and/or interferon therapy. Physicians and ophthalmologists should be alert to this potential but infrequent association as the resultant visual loss is a significant potential complication that should be discussed when obtaining informed consent for interferon treatment.
Keywords: Hepatitis C, interferon alpha, cystoid macular edema, visual loss
Hepatitis C, virus (HCV) may be associated with an ischemic retinopathy thought to be secondary to HCV-induced vasculitis.[1] Contemporary treatment for chronic systemic HCV infection comprises interferon alpha in combination with ribavirin. The side-effects of interferon include a flu-like illness, fever, fatigue, nausea, hair loss and depression. Interferon treatment has been associated with a retinopathy, characterized by cotton wool spots and retinal hemorrhages, in several prospective case series and has also been reported to cause Vogt-Koyanagi-Harada disease.[2–6] Despite this, patients rarely report subjective visual problems and visual function is generally maintained.
Here we present optical coherence tomography (OCT) evidence of cystoid macular edema (CME) probably due to pegylated interferon alpha treatment for hepatitis C in an otherwise healthy individual with none of the common risk factors for CME. To our knowledge, only two similar cases of this rare and emerging phenomenon have previously been reported worldwide
A 48-year-old white male was referred to the ophthalmic accident and emergency by his general practitioner. He gave a six-month history of gradual, painless loss of central vision in his left eye. Visual acuities were 20/16 in the right eye unaided and 20/400 best corrected in the left eye. Both eyes were white with no intraocular inflammation and left eye CME was confirmed on slit-lamp biomicroscopy. Furthermore, OCT showed three symmetric cystic spaces in the external plexiform layer, increased free space between the neurosensory epithelium and retinal pigmented epithelium and disorganization of internal retinal architecture at the macula [Fig. 1]-consistent with the clinical diagnosis of CME.
Fundus photographs and optical coherence tomography scans at first presentation showing cystoid macular edema of the left eye

Topical treatment was commenced in the form of ketorolac 0.5% eye drops four times daily and dexamethasone 0.1% eye drops four times daily to the left eye. At the three-month follow-up he reported no subjective improvement in vision and acuity remained poor at 20/200 despite a repeat OCT scan showing resolution of edema. Fundus fluorescein angiogram and fundus autofluorescence confirmed macular retinal pigment epithelial atrophy. Active management and further follow-up were declined by the patient.
The incidence of retinopathy associated with interferon treatment varies in literature from 18-86%.[1] The most common lesions seen are cotton wool spots and retinal hemorrhages and actual subjective visual complaints or documented visual loss is infrequent. Our case is highly unusual in both the pathology and also in terms of the level of visual loss. Such ocular side-effects or associations are extremely rare and whilst routine ophthalmic screening at baseline and through the course of peg-IFN-alpha and ribavirin therapy may not be indicated, this case demonstrates that early ophthalmic assessment and treatment in the event of subjective decrease in vision may improve the final visual prognosis.
Hypertension and diabetes mellitus have been shown to be risk factors in the development or progression of interferon-associated retinopathy in HCV-infected individuals. However, neither was identified in our patient.
In summary, we present a rare case of CME with attendant visual loss which may be causally related to interferon alpha treatment of hepatitis C. Ophthalmologists and physicians should be aware of the possible ocular side-effects of interferon and whilst treatment of the systemic disease must take priority, we suggest that the potential for transient or longer-term visual loss be discussed when obtaining informed consent for interferon therapy.
1. Zegans ME, Anninger W, Chapman C, Gordon SR. Ocular manifestations of hepatitis C virus infection. Curr Opin Ophthalmol. 2002;13:423–7. [PubMed]
2. McHutchinson JG, Poynard T. Combination therapy with interferon plus ribavirin for the initial treatment of chronic hepatitis C. Semin Liver Dis. 1999;19:57–65. [PubMed]
3. Kawano T, Shigehira, Uto H, Nakama T, Kato J, Hayashi K, et al. Retinal complications during interferon therapy for chronic hepatitis C. Am J Gastroenterol. 1996;91:309–13. [PubMed]
4. Schulman JA, Liang C, Kooragayala LM, King J. Posterior segment complications in patients with hepatitis C treated with interferon and ribavirin. Ophthalmology. 2003;110:437–42. [PubMed]
5. Hayasaka S, Nagasaki Y, Matsumoto M, Sato S. Interferon associated retinopathy. Br J Ophthalmol. 1998;82:323–5. [PMC free article] [PubMed]
6. Kasahara A, Hiraide A, Tomita N, Iwahashi H, Imagawa A, Ohguro N, et al. Vogt-Koyanagi-Harada disease occurring during interferon alpha therapy for chronic hepatitis C. J Gastroenterol. 2004;39:1106–9. [PubMed]
7. Tokai R, Ikeda T, Miyaura T, Sato K. Interferon-associated retinopathy and cystoid macular oedema. Arch Ophthalmol. 2001;119:1077–9. [PubMed]
8. Shimura M, Saito T, Yasuda K, Tamai M. Clinical course of macular oedema in two cases of interferon-associated retinopathy observed by optical coherence tomography. Jpn J Ophthalmol. 2005;49:231–4. [PubMed]
.
Journal of Pediatric Gastroenterology & Nutrition:
August 2010 -
doi: 10.1097/MPG.0b013e3181b99cf0
Original Articles: Hepatology and Nutrition
Ophthalmologic Complications in Children With Chronic Hepatitis C Treated With Pegylated Interferon
Narkewicz, Michael R
Abstract
Objectives: Interferon treatment for chronic viral hepatitis C (HCV) has been associated with the development of retinopathy in 19% to 29% of adults. Our purpose is to describe the ophthalmologic complications of pegylated interferon-α2a with either placebo or ribavirin in children with chronic HCV (the PEDS-C trial).
Materials and Methods: Prospective, comprehensive ophthalmologic examinations including slit lamp at enrollment and after 24 and 48 weeks of treatment of 114 children participating in a randomized clinical trial.
Results:
Conclusions: Ophthalmologic complications are infrequent in children who are treated with pegylated interferon-α2a for HCV (2%–3%). Because of the potential severity of ischemic retinopathy and uveitis, prospective ocular assessment should remain part of the monitoring strategy for children who are treated with interferon for HCV
Four weeks prior to this visit, the patient was seen in our eye clinic at the University of Iowa for a history of floaters and a few episodes of “prisms of light” in both eyes lasting for 5 to 10 seconds. His examination at that time, which included a detailed funduscopic examination, was unremarkable.
Past Medical History: Hepatitis C virus, tobacco use
Medications: Erythropoetin, peginterferon, ribavirin
Allergies: No known drug allergies
Family and Social History: Non-contributory
Slit Lamp Examination:
OD: 20/20-2
OS: 20/40, with pinhole 20/20
IOP: 12mmHg OD, 11mmHg OS
Pupils: 3 mm -> 2 mm, brisk, equal with no relative afferent pupillary defect
Confrontation visual field: Full OU
Extraocular movements: Full OU
External exam: Normal OU
Slit lamp exam:
Lids/lashes: Normal OU
Conjunctiva: Normal OU
Sclera: Normal OU
Cornea: Clear OU
Anterior chamber (AC): Deep and quiet OU
Iris: Normal OU
Lens: 1+ nuclear sclerosis OU
Vitreous: Clear OU, no Shafer’s sign OU
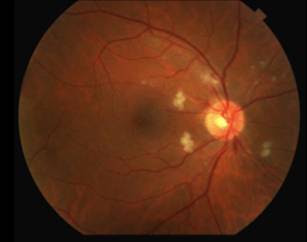
Dilated Fundus
Disc: pink, sharp borders, multiple cotton wool spots (CWS) surrounding the nerve, small areas of retinal hemorrhages around the nerve OU
Cup to disc ratio: 0.3 OU
Macula: flat OU, few CWS encroaching upon the macula OU
Vessels: normal OU
Periphery: normal OU
Left Eye

Discussion:
The differential diagnosis for diffuse CWS surrounding the optic nerves in both eyes (Figure 1) includes: interferon-associated retinopathy, hypertensive retinopathy, retinopathy associated with leukemia/lymphoma, ocular ischemia, Purtcher's retinopathy (insert link to our Eyerounds case) and HIV retinopathy.
Given that the patient had recently started interferon therapy, was HIV negative, had a normal blood pressure and blood cell count and had no risk factors for ocular ischemia or Purtcher’s retinopathy, the most likely diagnosis was interferon-associated retinopathy.
Many reports have discussed the ocular complications associated with interferon use as an antiviral or antiangiogenic agent. Ikebe first reported this condition in a 39-year-old gentleman who developed retinopathy after administration of intravenous interferon (Ikebe et. al. 1990). Other complications associated with interferon include ischemic optic neuropathy, subconjunctival hemorrhage, retinal hemorrhage, combined choroidal and retinal perfusion deficits and cystoid macular edema (Guyer et. al. 1993, Schulman et. al. 2001, Tokai et. al. 2001). Interferon associated retinopathy occurs in 19% to 69% of adults on interferon therapy (Narkewicz et. al. 2010, Schulman et. al. 2001).
Interferon-associated retinopathy often presents with cotton wool spots, retinal hemorrhages and other retinal microvascular irregularities (Esmaeli et. al. 2001).
Frequent monitoring of patients on interferon is important. Patients with normal exams should be followed every 4 to 6 months while those with retinopathy should be followed more frequently while on treatment.
However, after only 6 weeks of treatment (around the same time that the retinopathy was noted), his viral load became undetectable. We were concerned about visual prognosis as the CWS were close to the macula, but the hepatology service, understandably, had hoped to continue treatment given its success.
Extensive discussions took place between the patient, his family and the hepatology and ophthalmology services. An attempt was made to weigh the potential risk to the eye against the significant benefit of decreased viral load and activity of HCV while on peginterferon. After careful deliberation, the patient decided to continue with the HCV treatment for now, considering his great response thus far and the likelihood that he would not need to be on the treatment for an extended period of time. The ophthalmology service agreed to closely monitor the patient for CME and other signs of worsening interferon-associated retinopathy.
Figure 2:
Left Eye

Right Eye

Diagnosis: Interferon-associated Retinopathy
No age/gender predilection
Pre-existing arteriosclerosis that affects microcirculation may promote development of retinopathy
Cotton wool spots especially around the optic nerve
Retinal hemorrhages
Cystoid macular edema
Decreased visual acuity
Floaters
Most patients are asymptomatic
Cessation of interferon treatment
May require retinal consultation if complications arise
Interferon-associated retinopathy
Hypertensive retinopathy
Retinopathy from leukemia/lymphoma
Ocular ischemia
HIV retinopathy
References
Esmaeli, B., Koller, C., Papadopoulos, N., Romaguera, J. Interferon-induced Retinopathy in Asymptomatic Cancer Patients. Ophthalmology 2001;108:858-860.
Guyer, DR., Tiedeman, J., Yannuzzi, L., Slakter, J., Parke, D., Kelley, J., Tang, R., Marmor, M., Abrams, G., Miller, J., Gragoudas, E. Interferon-Associated Retinopathy. Arch of Ophthalmol 1993;111:350-356.
Ikebe, T., Nakatsuka, K., Goto, M. A Case of Retinopathy Induced by Intravenous Administration of Interferon. Folia Ophthalmol 1990;41:2291-2296.
Kadayifcilar, S., Boyacioglu, S., Kart, H., Gursoy, M., Aydin, P. Ocular Complications with High Dose Interferon-alfa in Chronic Active Hepatitis. Eye 1999;13:241-246.
Meltzer, D. Interferon Retinopathy: A Side Effect from the Treatment of Hepatitis C. Optometry 2008;79 320-321.
Narkewicz, MR., Rosenthal, P., Schwarz, KB., Drack, A., Margolis, T., Repka, MX. Ophthalmologic Complications in Children with Chronic Hepatitis C Treated with Pegylated Interferon. Journal of Pediatric Gastroenterology and Nutrition 2010; Published ahead of print. (PMID: 20512062)
Okuse, C., Yotsuyanagi, H., Nagase, Y., Kobayashi, Y., Yasuda, K., Koike, K., Iino, S., Suzuki, M., Itoh, F. Risk Factors for Retinopathy Associated with Interferon alpha-2b and Ribavirin Combination Therapy in Patients with Chronic Hepatitis C. World J Gastroenterol 2006;12:3756-3759.
Schulman, JA., Liang, C., Kooragayala, LM., King J. Posterior Segment Complications in Patients with Hepatitis C Treated with Interferon and Ribavirin. Ophthalmology 2003;110:437-41.
Tokai, R., Ikeda, T., Miyaura, T., Sato, K. Interferon-Associated Retinopathy and Cystoid Macular Edema. Arch Ophthalmol 2001;119:1077-1079.
suggested citation format:
Wes A, Hong ES, Oetting TA. Interferon-Associated Retinopathy: Communicating with Internal Medicine. EyeRounds.org. July 26, 2010; Available from: http://www.EyeRounds.org/cases/116-Interferon-Retinopathy.htm.
The University of Iowa Department of Ophthalmology & Visual Sciences, 200 Hawkins Dr., Iowa City, IA 52242-1091.
No comments:
Post a Comment