
Update
Thursday, June 29, 2017
Liver cirrhosis: a risk factor for gallstone disease in chronic hepatitis C patients in China
Thursday, June 29, 2017
Liver cirrhosis: a risk factor for gallstone disease in chronic hepatitis C patients in China
Sunday, February 19, 2017
Also See 2011;
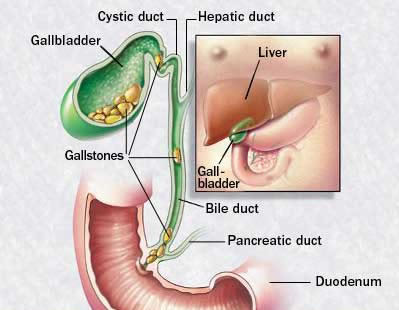
Where Is The Gallbladder & What Does It Do?
.It is pretty well surrounded by the liver in the upper right side of the abdomen under the rib cage and has small fluid line called a bile duct connecting it to the liver, pancreas and duodenum. The GB muscle which attaches to the rib cage produces powerful contraction when irritated.
Basically, it's just a sack that holds fluid composed of water, bile salts & cholesterol. When it comes out of the liver it is primarily water. The gallbladder just stores it until 95% of the water is drained away and then ejects it into the duodenum through the bile duct.
However, whether from the liver or gallbladder, bile primarily consists of the following substances: water, bile salts, bilirubin, cholesterol, fatty acids, lecithin, sodium and proteins. If the chemical balance of bile contains too much of any of these components, particularly cholesterol, crystals form and harden into gallstones. Cirrhosis causes the abnormal metabolism of bile pigment. Because of this, gallstones develop twice as often in cirrhosis patients as in those without the disorder. Cirrhosis prevents bile from flowing freely to and from the gallbladder, the bile hardens as gallstones. Cirrhosis poses a major risk for gallstones, particularly pigment gallstones. "Pigment stones are composed of calcium bilirubinate, or calcified bilirubin. Pigment stones can be black or brown, black stones form in the gallbladder and are the more common type. They represent 20% of all gallstones in the U.S. They are more likely to develop in people with hemolytic anemia (a relatively rare anemia in which red blood cells are destroyed) or cirrhosis (scarred liver)". ,
The pain is a result of the gallbladder's large, powerful muscle which is attached to the rib cage, and is contracting in an effort to release bile into the duodenum to neutralize the acid from the stomach. Thus, a stone anywhere in the bile duct, from the liver's exit to the gallbladder's or the pancreas (which shares a common bile duct). Is capable of producing deathlike pain.
The risk factor for women is greater then in men to develop gallstones. In women gallstones occur by the age of 60 in 25% of women and 50% by age 75. Women may be at an increased risk because estrogen stimulates the liver to remove more cholesterol from blood and divert it into the bile. Risk factors in men are about 20% by the age of 75. Because most cases do not have symptoms the rates may be underestimated in elderly men. In people with diabetes there is a higher risk for gallstones and have a higher-than-average risk for acalculous gallbladder disease (without stones). Gallbladder disease may progress more rapidly in patients with diabetes, who tend to have worse infections.
Risk for gallstones are also seen in transplantation, bone marrow, and solid organ transplant. The complications can be so severe that some organ transplant centers require the patients gallbladder be removed before the transplant is performed.
Research has shown that Hepatitis C patients have a greater tendency to develop gallstones. This takes the form of inflammation and pain with or without gallstones causing nausea and possibly vomiting. As a result some people with hepatitis C may have their gallbladder removed. A study in the Journal of Viral Hepatitis last year demonstrated that chronic HCV patients without cirrhosis have an increased prevalence for gallstones.
Data from the 2009 study as published in Medscape :
"Compared with the controls, gallstone disease is present in HCV patients at a younger age and in association with central obesity and liver steatosis, and is not related to gallstone heredity, dyslipidaemia, diabetes mellitus or metabolic syndrome. Although we could not establish a temporal relationship, the association between HCV infection and gallstone disease is real and appears to be causally linked at least in predisposed individuals, namely obese and with liver steatosis".
.See Full Study: Hepatitis C Virus Infection is a Risk Factor for Gallstone Disease: A Prospective Hospital-based Study of Patients with Chronic Viral C Hepatitis
Video
Gallstones are solid deposits of cholesterol or calcium salts that form in your gallbladder or nearby bile ducts. Complications from gallstones can be serious, and even fatal, if left untreated. Learn about the different causes, symptoms, and treatments of gallstones in this video.
By David King M.D.
Learning about the Gallbladder and Bile System
Anatomy and Function.
Anatomy and Function.
The biliary system essentially consists of the liver, the bile ducts, the gallbladder and the ampulla of Vater. Biles main function is to aid in the absorption and digestion of fats. Bile is made by the liver and then secreted into tiny tubes or ducts in the liver. The bile then travels through these small ducts within the liver, join other ducts within the liver and eventually exiting the liver and becoming one large duct outside called the common hepatic duct. This portion of the bile system is sometimes called the “biliary tree” because the way it resembles a tree with leaves, twigs and branches that eventually all combine to form a common trunk.
The gallbladder is a hollow, pear-shaped, muscular “bag” that has one opening through another duct called the cystic duct. The cystic duct eventually meets the common hepatic duct where they join to form the common bile duct. This duct continues on to join the duodenum (the first part of the small intestine) through a structure called the ampulla of Vater. Within this structure is a muscle “valve” called the sphincter of Oddi which prevents the flow of bile into the small intestine except at specific times.

The liver makes about a quart of bile over the course of an entire day but the body only uses a significant amount of bile when food is present in the duodenum. Because of this, the flow of bile is diverted into the gallbladder during most of the day. Since the gallbladder can only hold about ¼ cup of fluid, it has a remarkable ability to concentrate the bile and reduce its volume by as much as 90%. When food reaches the duodenum after being eaten, the body releases a hormone called cholecystokinin (CCK) which stimulates the sphincter of Oddi to open and the gallbladder wall to contract which squirts the stored, concentrated bile into the duodenum where it mixes with the food to aid in absorption and digestion
.
.Gallbladder Disease
The presence of gallstones is a very common condition that can lead to gallbladder disease. During the concentration of bile, small cholesterol particles can come out of solution and form a layer of sludge within the gallbladder. If this sludge does not get completely evacuated from the gallbladder during contraction it can gradually build up over time. The sludge will usually separate into clumps that eventually become stones. Sometimes many smaller stones are formed and at other times one or two very large stones may form. If these stones become large enough to block the cystic duct when the gallbladder contracts they can inhibit the flow of bile from the gallbladder.
This can lead to the classic symptoms of pain in the right, upper abdomen with associated nausea or vomiting shortly after eating a meal. Since the stones are freely floating within the gallbladder, they may not block the flow of bile with every meal and symptoms may only occur intermittently. If a stone becomes impacted in the neck of the gallbladder, symptoms may become severe and constant requiring urgent intervention to obtain relief. Occasionally, smaller stones may pass through the cystic duct and reach the common bile duct during a gallbladder contraction.
.These stones may pass harmlessly into the small intestine through the ampulla of Vater.
However, if they become impacted at the sphincter of Oddi they can cause life-threatening conditions such as pancreatitis or cholangitis.

Even without the formation of stones, a gallbladder may produce symptoms when it fails to contract properly when stimulated by CCK. A normal gallbladder will eject most of the bile it contains when stimulated. When a gallbladder can only eject 35% or less of its volume with each contraction it is considered diseased. In this condition, the typical gallbladder symptoms of right-sided upper abdominal pain, nausea and vomiting will often be present constantly but with less severity than with gallstones
.
.Diagnosis
. Gallstones may be diagnosed most easily with ultrasound. Because the stones are higher in density than the surrounding tissue and bile they will absorb or reflect more sound waves leaving a “shadow” on the ultrasound screen. CT scans and plain x-rays will not usually show gallstones unless they contain significant amounts of calcium
. Gallstones may be diagnosed most easily with ultrasound. Because the stones are higher in density than the surrounding tissue and bile they will absorb or reflect more sound waves leaving a “shadow” on the ultrasound screen. CT scans and plain x-rays will not usually show gallstones unless they contain significant amounts of calcium
.
HIDA Scan
If a patient has typical gallbladder symptoms but their ultrasound does not show any stones a HIDA scan may be ordered. This study involves the placement of an intravenous catheter and injection of a non-harmful radioactive substance that is gathered up by the liver and secreted into the bile. A special type of camera that recognizes radioactive waves is then used to visualize the liver and the gallbladder. Once the gallbladder is full of the radioactive bile, its volume is calculated and a second injection of the hormone CCK is performed through the same intravenous catheter. The volume of the gallbladder is again determined and compared to its full volume. The difference in these two volume measurements is calculated by the physician reading the study and expressed as a percentage number called the ejection fraction. An ejection fraction less than 35% is an indication that the gallbladder is not functioning properly.
Treatment
Many studies have been performed to determine if an effective medical treatment for gallstones exists. A drug was developed that is effective at dissolving gallstones but even when the gallstones were gone most patients still had symptoms. In most cases, the gallstones came back very rapidly after the medication was discontinued. This has lead most physicians to realize that once symptoms occur from gallstones the only proven effective treatment is surgical removal of the gallbladder. However, if gallstones are present but the patient has no symptoms then no intervention is needed in most cases. Surgical removal of the gallbladder remains the mainstay of gallbladder disease treatment. Over the past 15 years, laparoscopy has become the preferred method for gallbladder removal. Today, over 95% of gallbladder removal operations performed in the United States are completed laparoscopically. Most of these patients go home on the same day as their operation.
Gallbladder Removal Laparoscopic PreOp® Patient Education Feature
For this procedure, a surgeon typically uses 3 or 4 small incisions, a video camera and specialized instruments to remove the gallbladder from the cystic duct and the undersurface of the liver. Since the gallbladder mostly contains fluid, it can usually be removed from the abdomen through an incision no larger than ½ inch. Occasionally, a larger incision must be made when a large stone or multiple stones are present. In a few instances, laparoscopic removal of the gallbladder cannot be performed safely and open surgical technique is required. Sometimes an unanticipated situation or complication found during laparoscopic gallbladder surgery may require conversion to open surgical technique as well.
Open surgery usually requires a longer hospital stay and is typically more painful due to the presence of a large incision. Major complications of gallbladder surgery occur in less than 5% of patients by most recent studies.
Homeopathic
“gallstone-cleansing” techniques have been proclaimed effective and safe by many homeopathic practitioners and lay-people. These treatments usually involve the ingestion of significant quantities of olive oil and citrus juice in an attempt to cause vigorous contraction of the gallbladder to eject all of the stones into the small intestine. Some remedies include a special pectin rich diet for several days before the cleansing which has been shown in some animal studies to soften gallstones. Though these remedies may have been helpful for some people there have been no human studies to confirm its effectiveness or document the risks. Since life-threatening conditions such as pancreatitis and cholangitis can occur with passage of gallstones, these risks should be fully considered before trying any homeopathic remedy.
After Gallbladder Removal
Most patients are eventually able to tolerate any foods they enjoy after their gallbladder has been removed. However, many patients will experience problems such as nausea, bloating and diarrhea with certain foods during the first few months following surgery. A few patients will experience these symptoms regardless of their diet during the first few months following surgery. A small percentage will have these symptoms persist and require significant diet changes, lifestyle modification or medication to manage their condition. Usually fried, greasy or spicy foods tend to cause the most symptoms but any food could become poorly tolerated following gallbladder surgery.
.Other Similar Conditions
Several other different diseases can cause symptoms similar to gallbladder disease. Irritable Bowel Syndrome (IBS), peptic ulcers, gastritis or gastroesophageal reflux disease (GERD) may all mimic symptoms of gallbladder disease. These diagnoses should be considered whenever gallbladder studies are normal but typical symptoms are present.
Conclusion Points
Gallstones are very common. Usually, only symptomatic gallstones need treatment. A poorly functioning gallbladder may also need treatment. Medical or homeopathic treatment has not been proven effective. Most patients are able to lead a normal life without their gallbladder. Surgical removal of the gallbladder is effective and carries a relatively low-risk for most patients.
Gallstones are very common. Usually, only symptomatic gallstones need treatment. A poorly functioning gallbladder may also need treatment. Medical or homeopathic treatment has not been proven effective. Most patients are able to lead a normal life without their gallbladder. Surgical removal of the gallbladder is effective and carries a relatively low-risk for most patients.
Gallstones can go unnoticed, but in some cases a stone could cause the gallbladder to become inflamed, resulting in pain, infection, or other serious complications.
If you already have been active Chronic Hepatitis C for over 14 Years and have no intention of Liver Transplant or any other Liver Treatments ie; Interferon and Ribavirin,(Combo), and failed treatment after undergoing 18 months of this treatment that was a nightmare to endure, can someone really explain why I should even think of having my Gaul Bladder removed. In my opinion it is futile.
ReplyDeleteAny suggestions from others that have already had this scenario would be appreciated.
I've had Chronic Hep C and Cirrhosis of the Liver for over 36 years. I have undergone treatment twice, 1 yr duration of Interferon and Ribaviran combo with negative results. I recently was blessed to participate in a 3 month trial based treatment using Harvoni and Ribasphere. The virus has been completely irraticated. I too have recently had problems with GS.and I'm planning on having the GB removed. My Liver Specialist stated it would be detrimental to end up in the ER. You really need to have a Surgeon and Liver Spec.colaberating together because of the high risk factors.
ReplyDeleteGood luck in whatever decision you make. Hope this has been helpful.